Detailed study of the 12 basic exercises
It is distressing to think that such a large deformity can appear in an otherwise healthy child, and that we still have no idea where it comes from.
JIP James, surgeon
 |
The Lyon method of non-surgical treatment of spinal deformity would evolve over the next 200 years as the extrapyramidal postural system was discovered and the biomechanics of deviation correction improved. To facilitate the training of physiotherapists, the 12 basic exercises resulting from a consensus among the major French-speaking scoliosis treatment centers will serve as the basis for teaching in physiotherapy schools. They are all the more useful as treatment becomes increasingly ambulatory and close to the patient. |
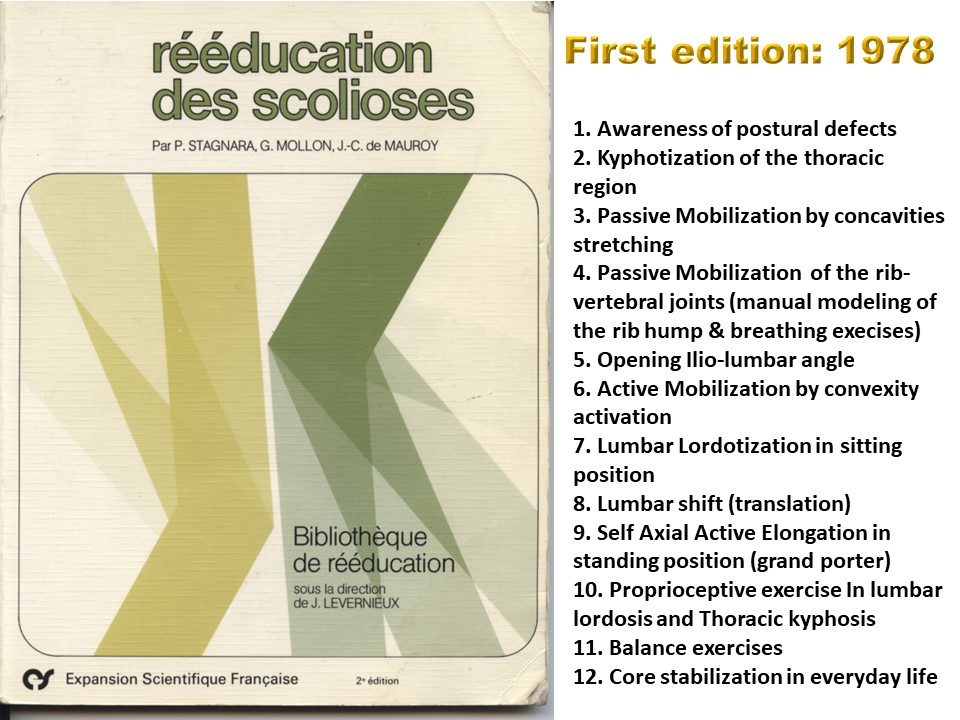 |
The first edition dates back to 1978, and was presented in Lyon during the "Scoliosis Days", attended by over 1,000 participants from all over Europe. Even if numerous indications concerning the indication, mode, intensity and duration of the exercises are provided, not all the characteristics of these execices were covered. |
 |
There are different ways of reading these exercises, and like the filters on a camera, we can study their different facets: anatomical, functional, neurophysiological, biomechanical... They also have a dimension of temporal progression. |
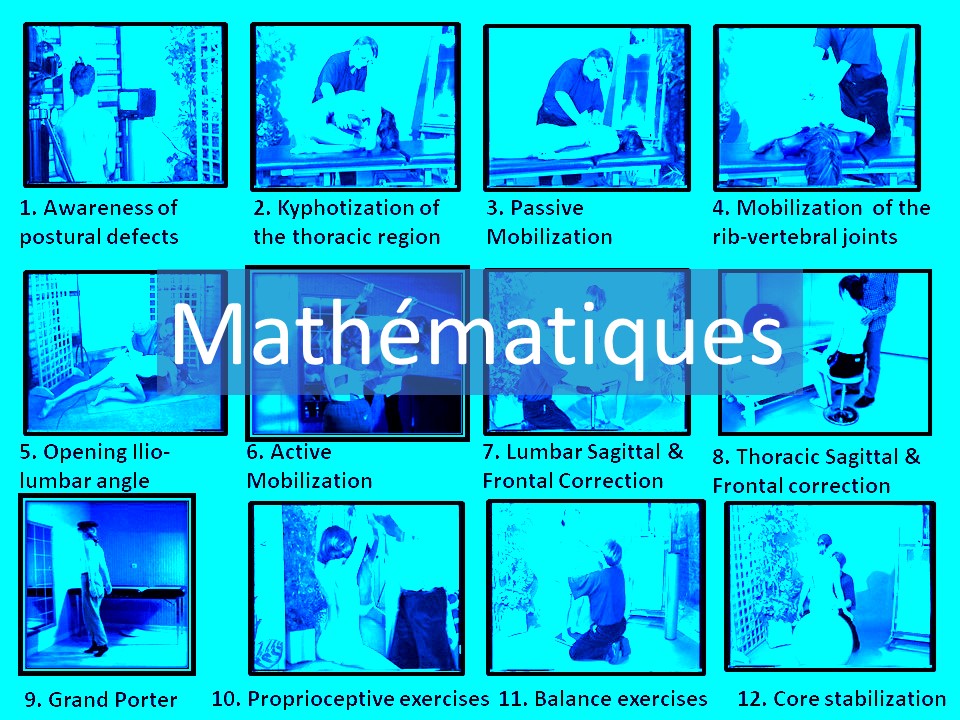 |
The number 12 is not a random number, and a mathematical introduction is the first step. 12 was widely used in the Middle Ages, as it was an easy way to count by pointing the thumb at the phalanges of the other 4 fingers. It also results from the division of the earth's year by the 12 lunations. |
 |
12 is a symbolic number, as it is one of the two sublime numbers. A sublime number is a natural integer whose divisors and sum of divisors are both perfect numbers its divisors (1, 2, 3, 4, 6 and 12) are 6, which is perfect; their sum, 28, is also a perfect number.
|
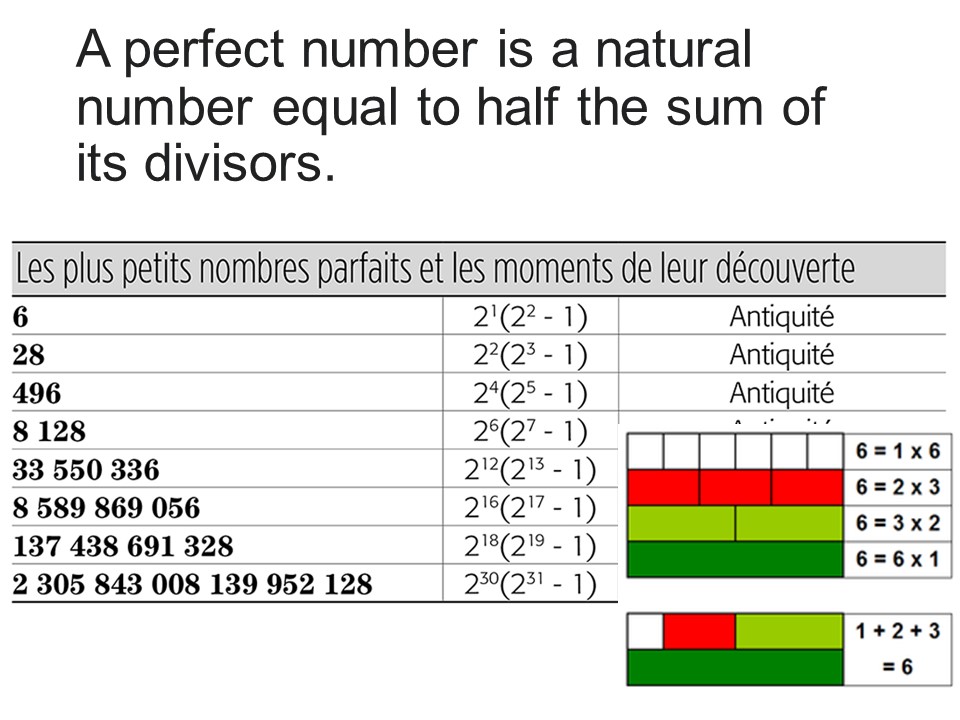 |
A perfect number is a natural integer equal to half the sum of its divisors. It's this mathematical perfection that makes it so easy to adapt the exercises to each patient. |
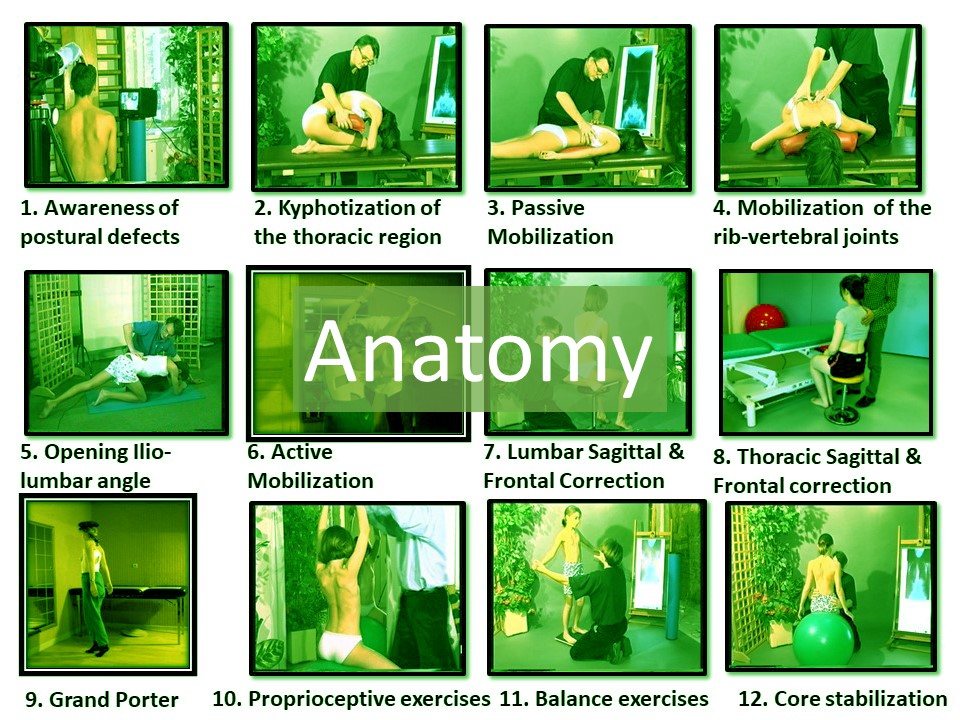 |
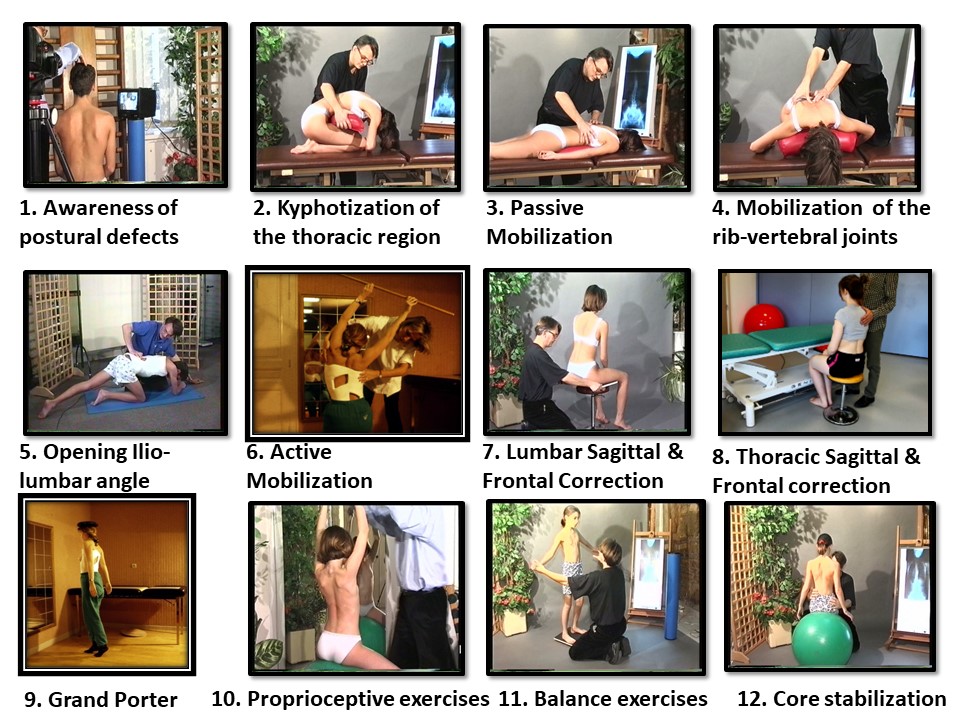
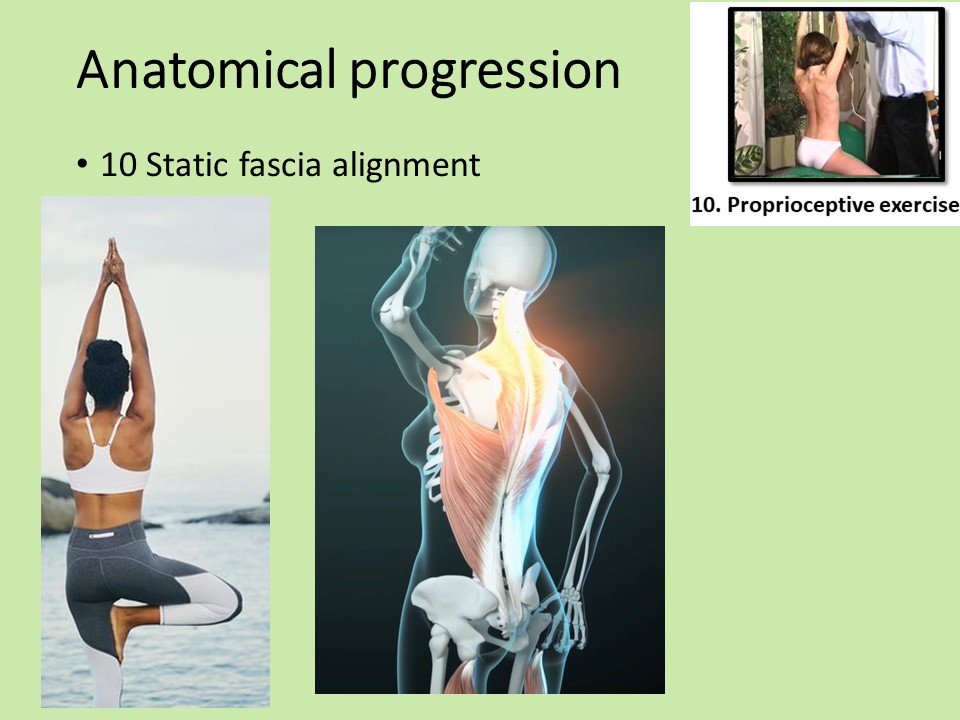
The first approach is anatomical. Each exercise addresses a specific structure in our body that will be used to correct the deviation. |
 |
The first exercise is to become aware of the deformation, which involves the mirror neuron system. They are the basis of learning by imitation. This is also the first contact between patient and physiotherapist, and these neurons play a role in empathy. |
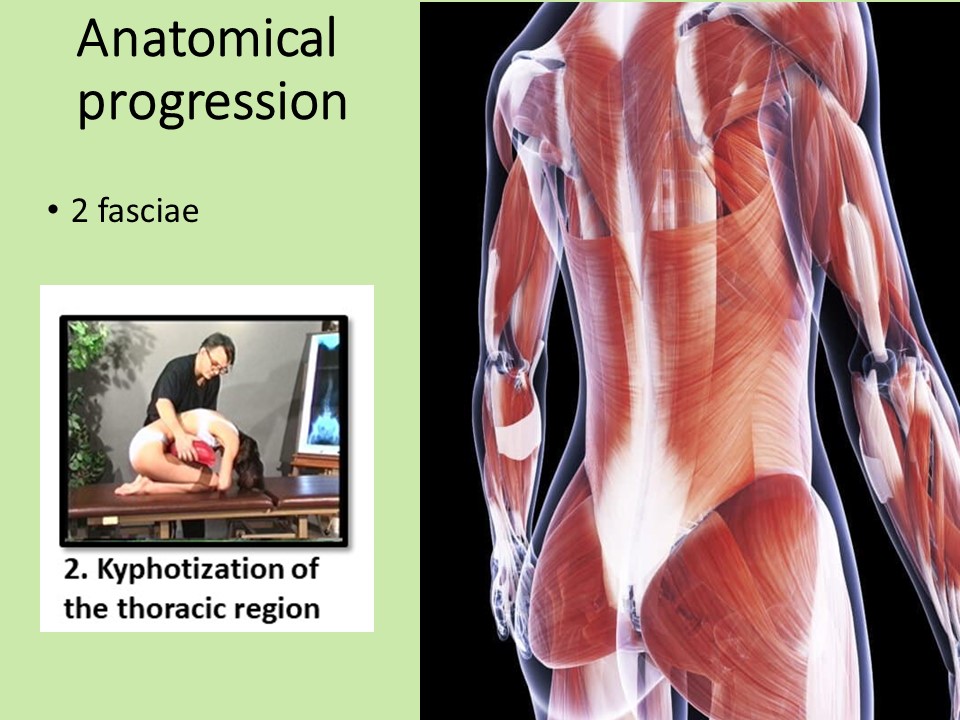 |
The second exercise involves stretching the posterior fasciae of the spine, which form a fundamental structural architecture and are asymmetrical in scoliosis. They cross at the thoraco-lumbar junction and are probably at the origin of thoraco-lumbar scoliosis.
|
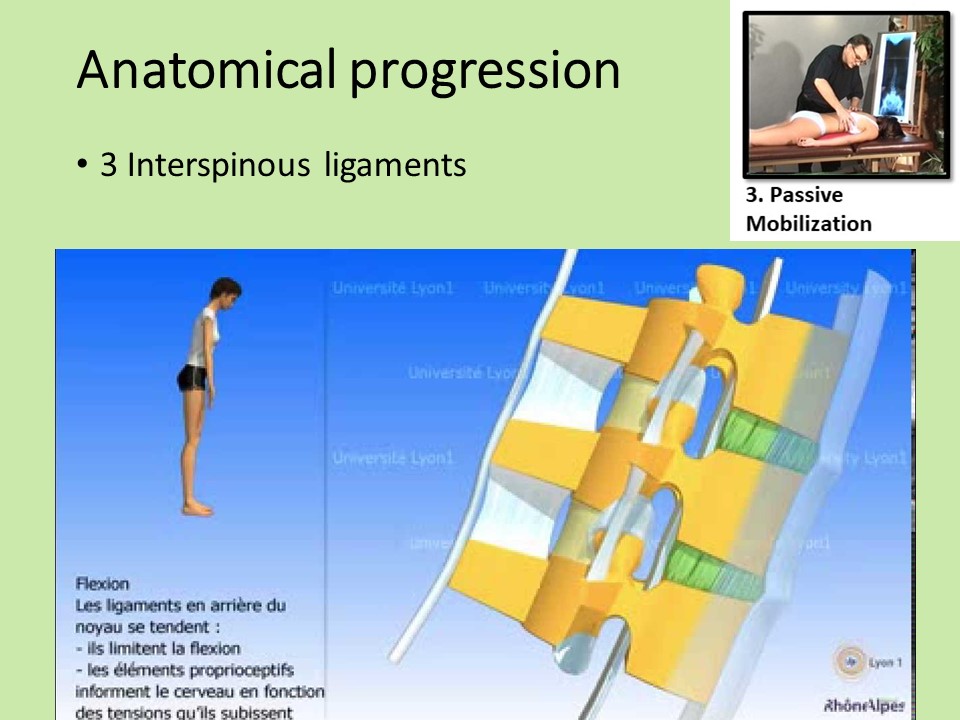 |
The third exercise involves the ligaments in the sagittal plane of function. Their tension is altered in scoliosis, disrupting their proprioceptive function. |
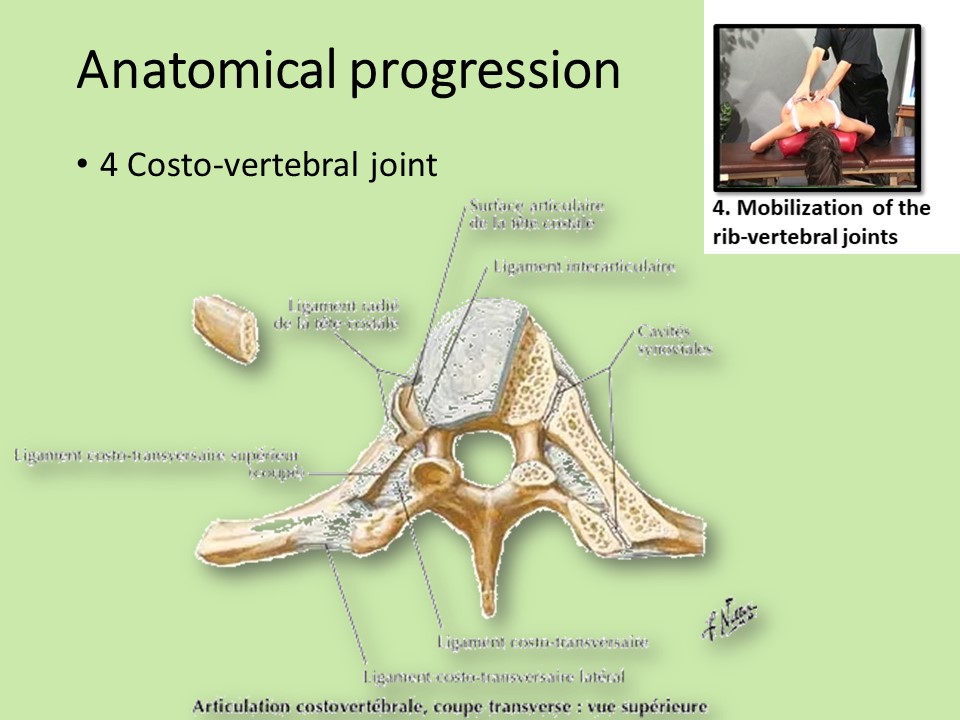 |
The fourth exercise concerns the costo-vertebral joints, which play a fundamental role in breathing. Their function is disrupted in scoliosis. Good mobility is essential for aerobic metabolism. |
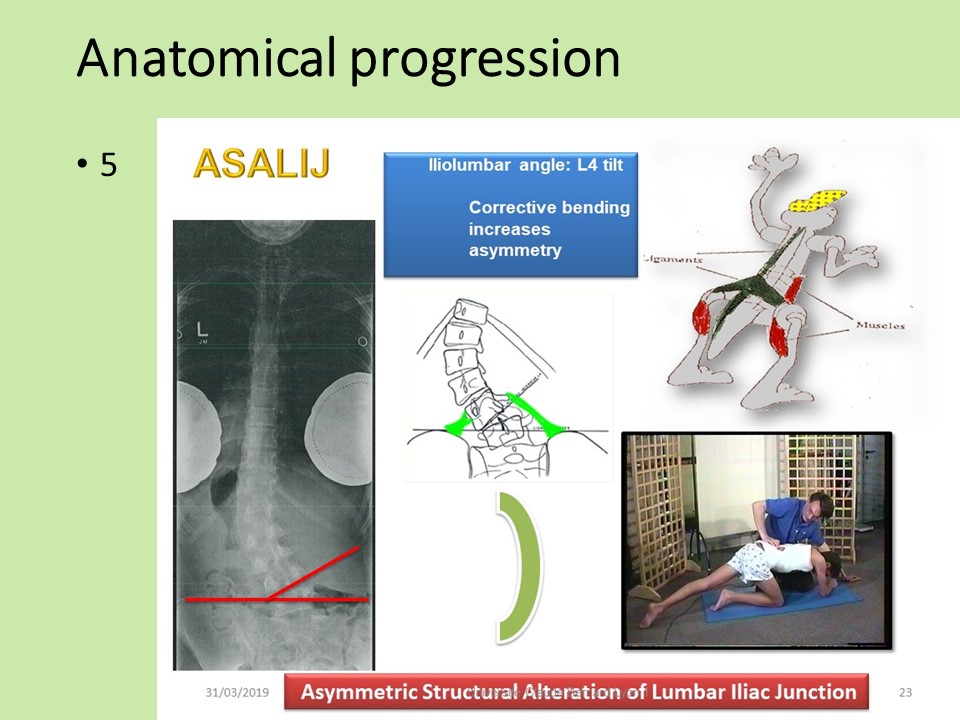 |
The fifth exercise concerns the lumbopelvic hinge, mainly in the case of L4 tilt. Structural abnormality of the lumbosacral hinge is a prerequisite for scoliosis correction. |
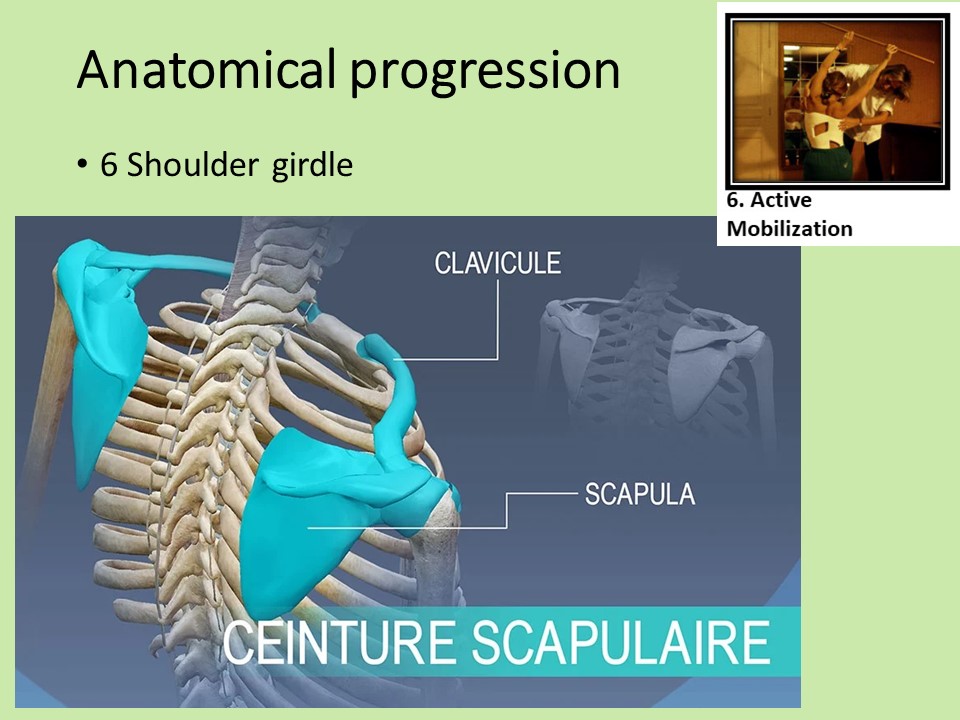 |
The sixth exercise concerns the shoulder girdle and the bony elements overlying the vertebral deviation. Shoulder imbalances are common in scoliosis, and are corrected so that the shoulder girdle forms the non-deformable base of the thoracic hyperboloid.
|
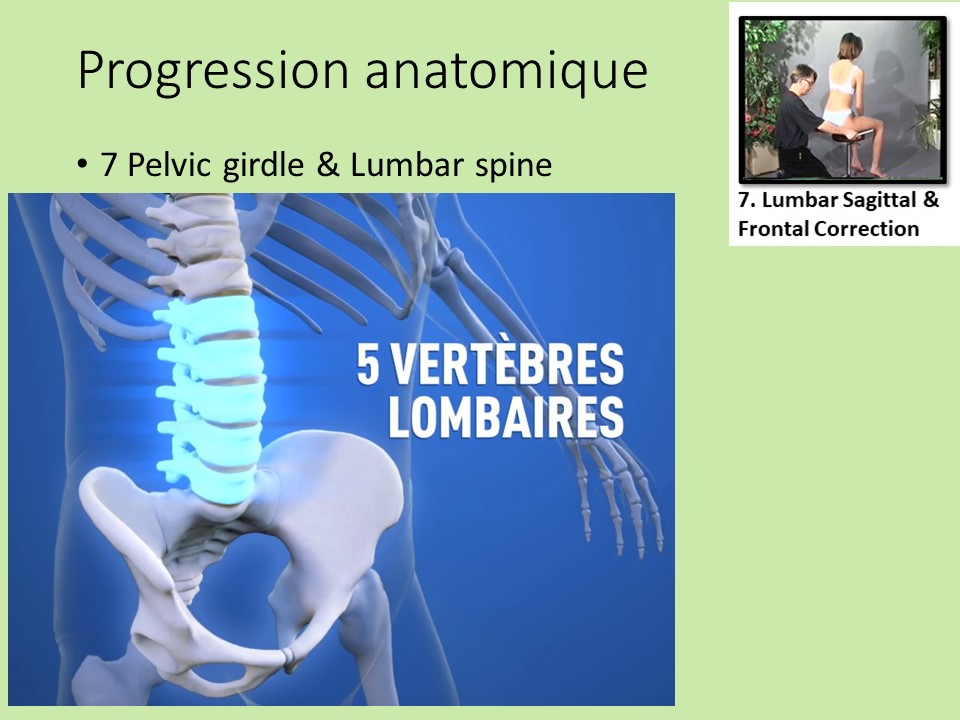 |
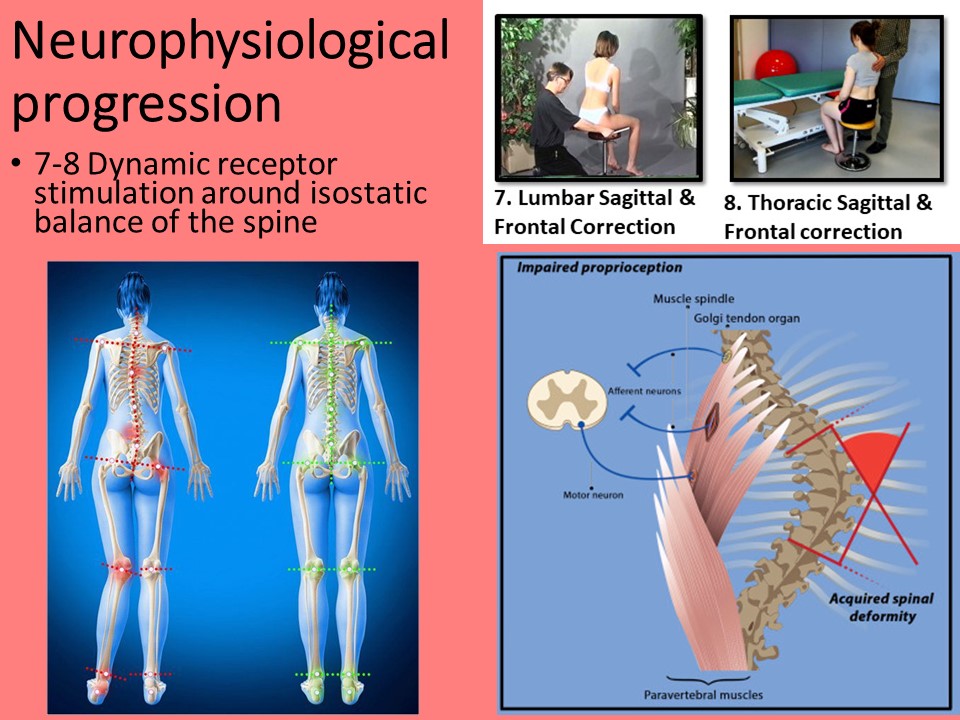
The seventh exercise concerns the lumbar region. The specific correction takes into account the sagittal orientation of the posterior facet joints. |
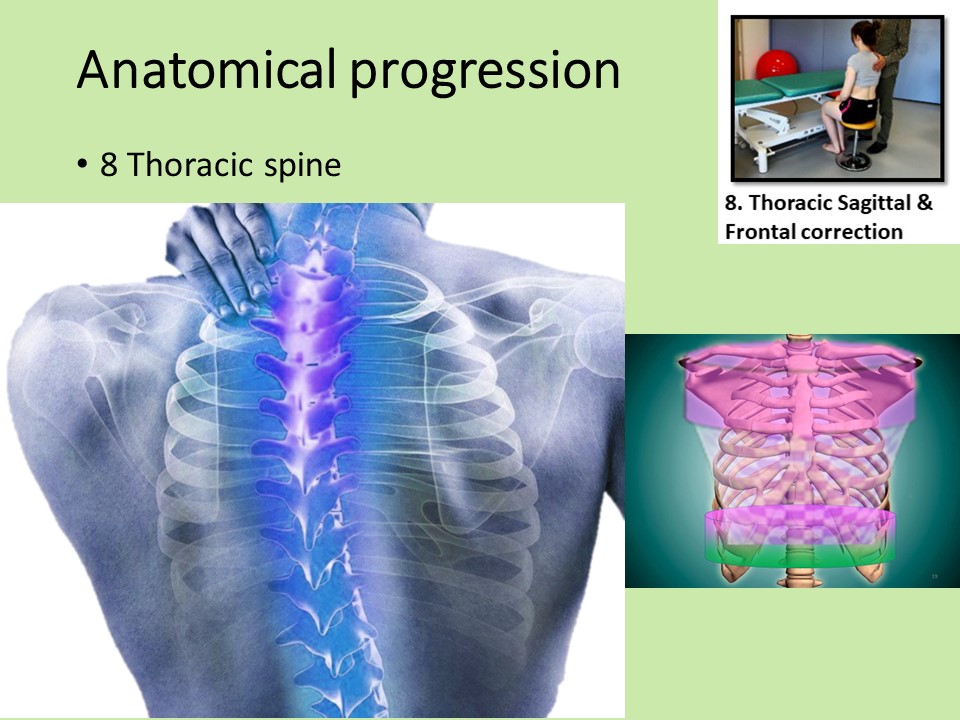 |
The eighth exercise concerns the thoracic region. The action on vertebral deviation is carried out via the thoracic hyperboloid. |
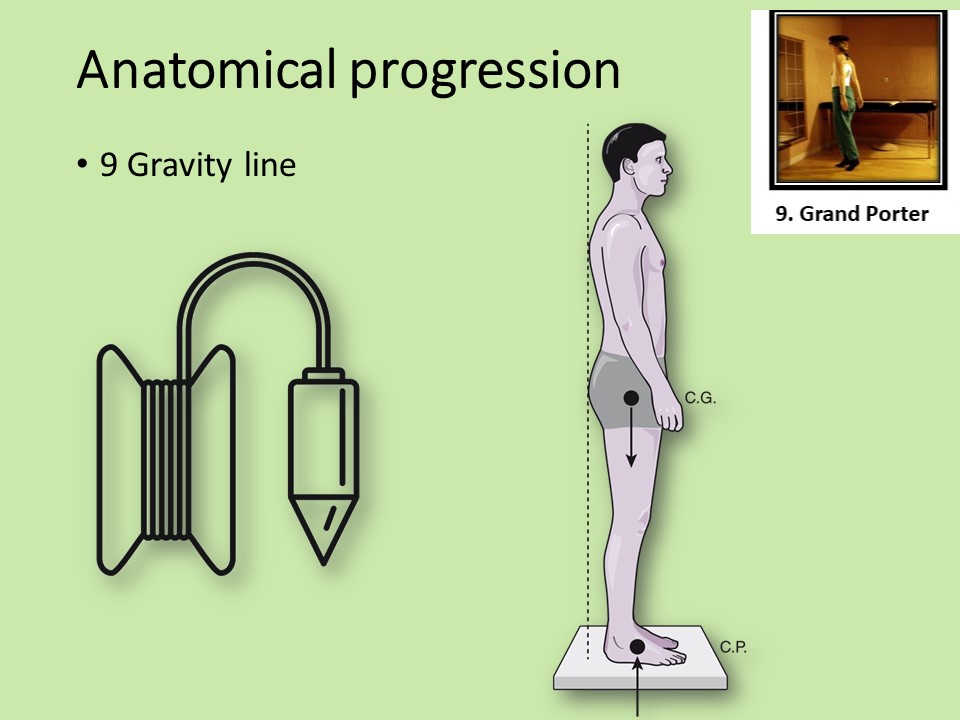 |
The ninth exercise is the most characteristic of the Lyon method. It involves the whole body aligned vertically along the line of gravity. |
 |
The tenth exercise, known as the rocket, raises the shoulder girdle automatically. From 90° to 150°: the upper trapezius fasciculus contracts to shorten itself by concentric contraction while the middle trapezius fasciculus lengthens with an eccentric contraction. The serratus major, abductor of the scapula, works with a concentric contraction. The anterior deltoid, long biceps and coracobrachialis continue their concentric contraction. Between 150° and 180°: the dorsal muscles come into play, such as the latissimus dorsi, which extends the dorsolumbar spine. dorsolumbar spine, as well as the trapezius, which extends the cervico-dorsal spine.
|
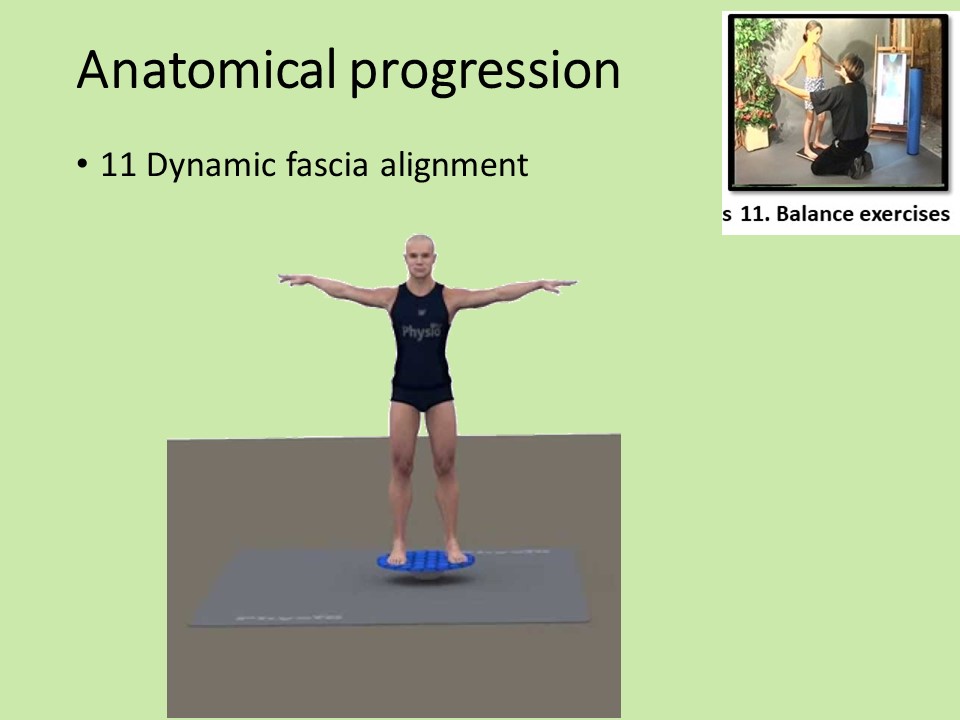 |
The eleventh exercise involves the entire spine, lower limbs and upper limbs, but in dynamic mode with podal instability. |
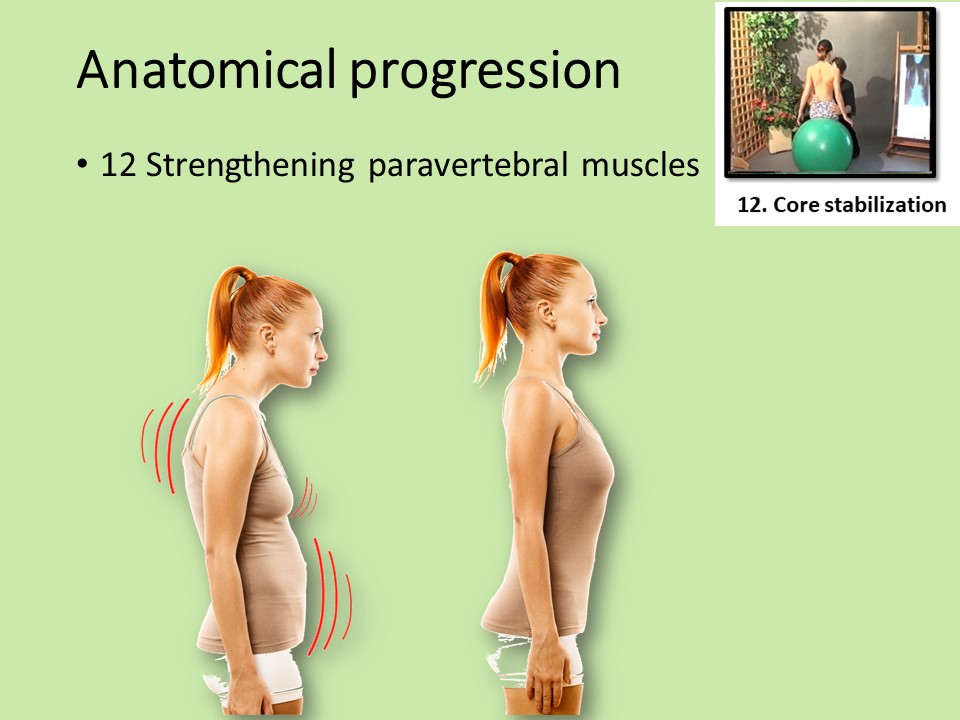 |
The twelfth exercise focuses on strengthening the paravertebral muscles. The core muscles are the adominals, pelvic floor, diaphragm and spinal extensors. |
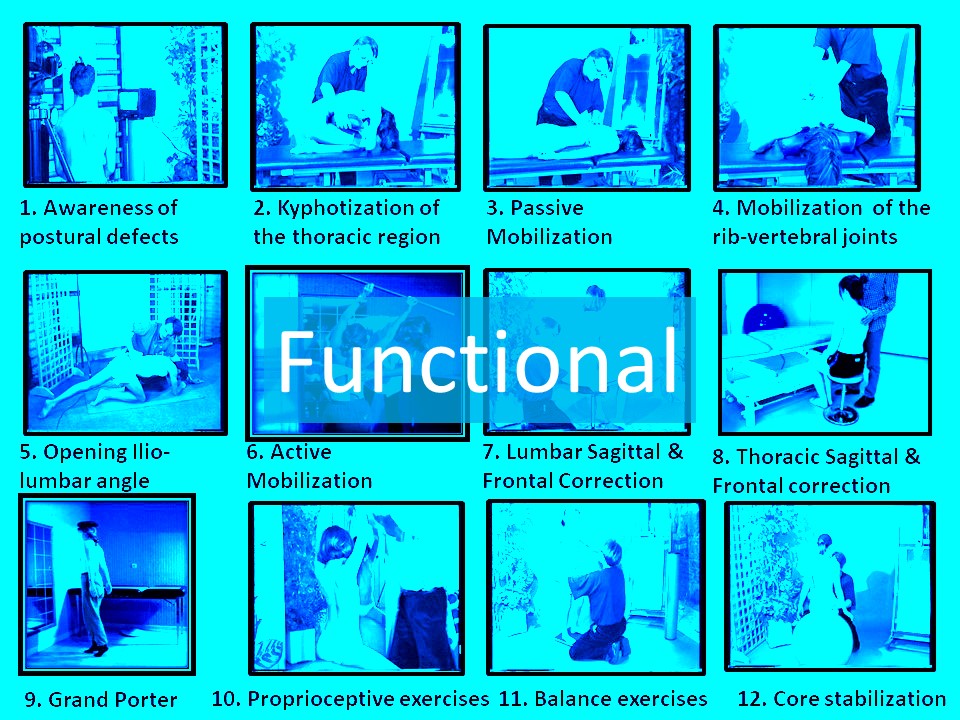 |
Each anatomical structure is called upon in a functional manner. |
 |
Mirror neurons are activated by seeing our own defects. Ideally, the physiotherapist should mime the desired correction. He or she can also add an external manual correction, enabling the patient to see the induced correction.
|
 |
The autonomic system managing vasodilation is stimulated by stretching the fascias. It's the equivalent of warming up before playing a sport. |
 |
Passive mobilization of medial ligament structures stimulates cutaneous proprioceptive receptors on the line of the spinous veins. When wearing a Lyon brace, these receptors are less stimulated because of the posterior bar. |
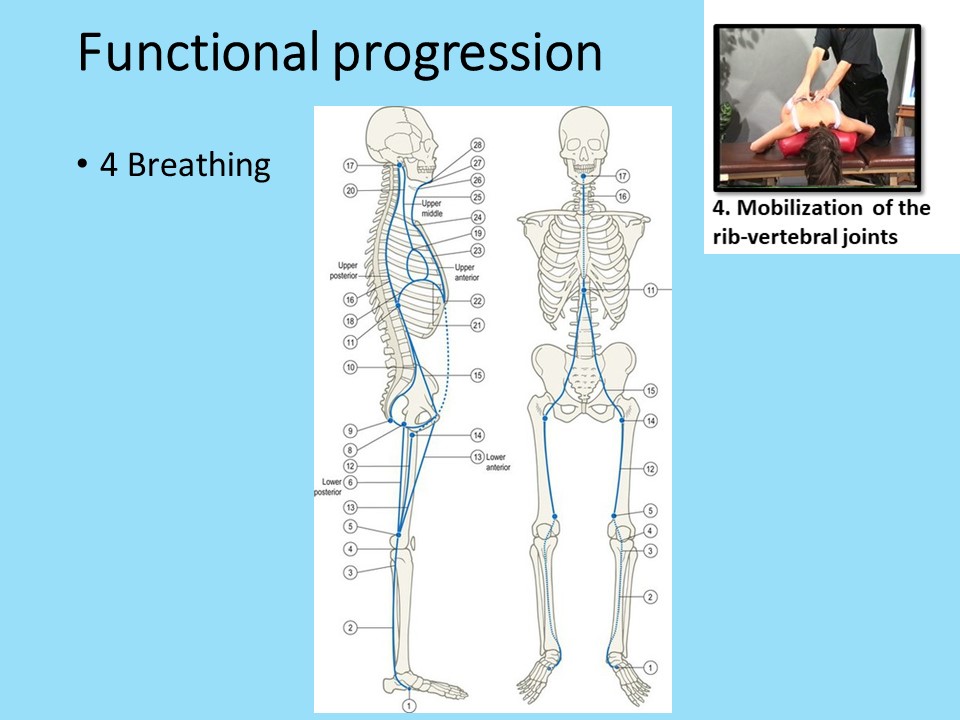 |
The links between the spine and breathing are very close. The diaphragm is part of the deep front line. Sagittal curvatures are diminished in inspiration, but increased in expiration. This is one of the reasons why the Lyon method emphasizes expiration. |
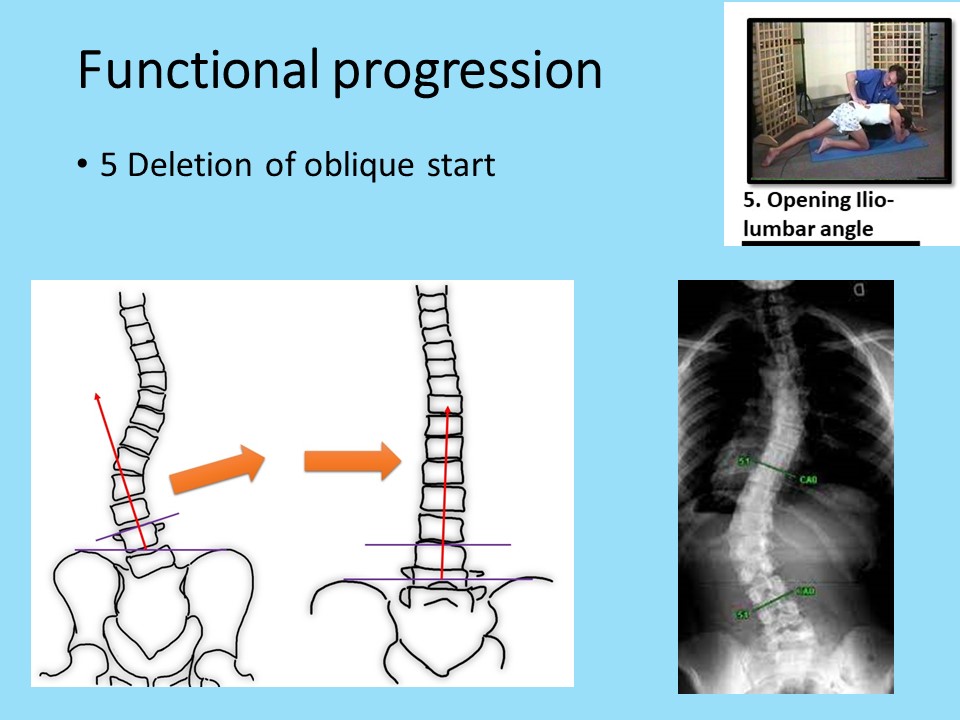 |
Opening the iliolumbar angle allows horizontalization of L4 and elimination of the oblique start
|
 |
Active mobilization of the shoulder girdle is essential for the dissociation of the girdles at the base of walking and running. |
 |
For the lumbar spine, 3D correction is performed in the sagittal plane in physiological lordosis, and in translation or shift in the frontal plane. Derotation in the horizontal plane is automatic via coupled movements. |
 |
For the thoracic spine, 3D correction is performed in the sagittal plane in physiological kyphosis, and in flexion or bending in the frontal plane. Derotation in the horizontal plane is automatic via coupled movements. |
 |
The grand porter is an all-round exercise. The small sandbag on the head stimulates balance and introduces a slight resistance to muscular action. As in exercise no.1, the mirror is used to check the dynamically corrected position.
|
 |
Proprioceptive receptors are sensitive to stretching and are stimulated by the rocket exercise. The aim is to maintain correction in the frontal plane in situations of slight imbalance due to pelvic instability in the sitting position. |
 |
In the standing position, balance is stimulated by instability of the foot. The exercise can be performed as a closed kinetic chain, with manual stabilization of the upper limbs, or as an open kinetic chain at home. |
 |
Vertebral deviation requires overall strengthening of the pyramidal and extrapyramidal musculature. |
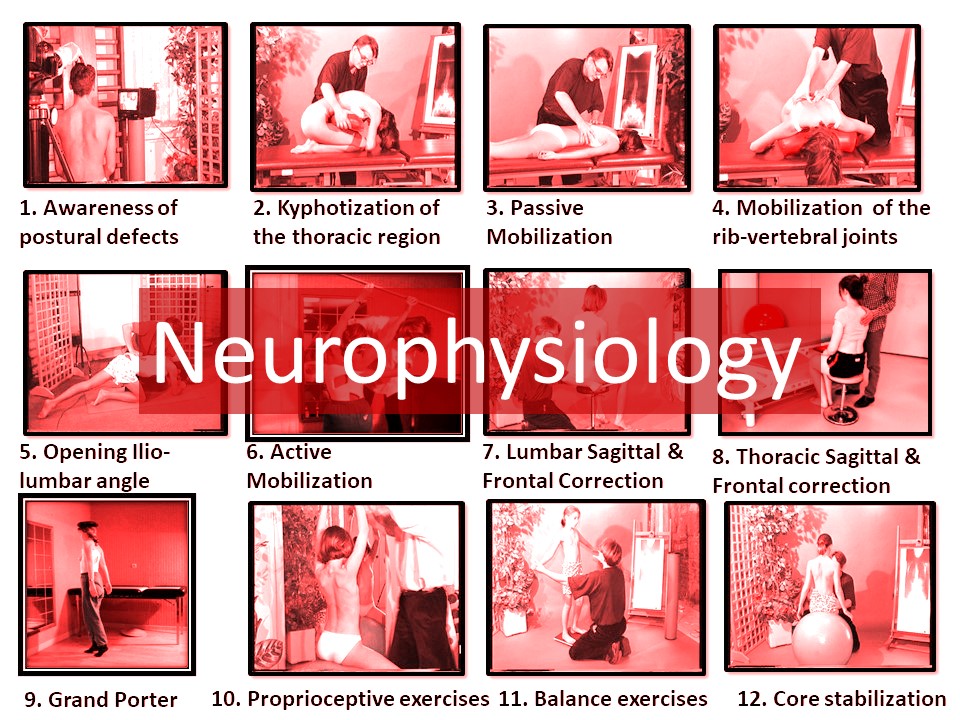 |
Idiopathic scoliosis is frequently associated with delayed maturation of the postural system (NOTOM). The third neurophysiological filter is characteristic of the Lyon method of stimulating the postural system.
|
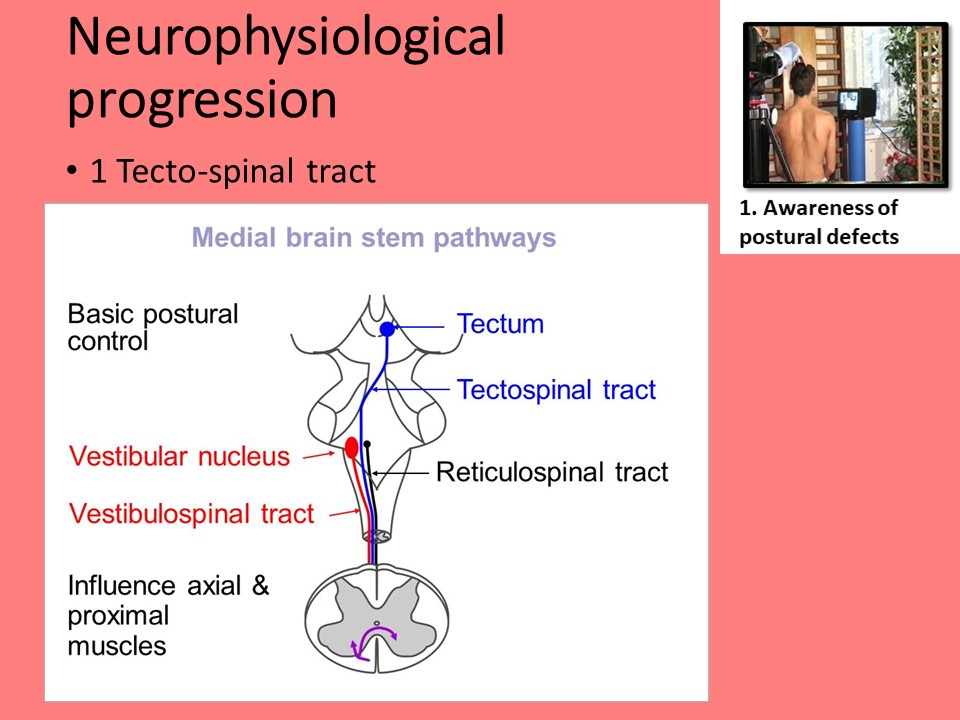 |
The mirror is widely used in scoliosis physiotherapy, just as it is indispensable in dance practice. You can see your back while keeping your gaze horizontal. It facilitates spatial perception. The inversion of laterality can be stimulating in the context of scoliosis. This exercise stimulates the tecto-spinal tract of the postural extra-pyramidal system. |
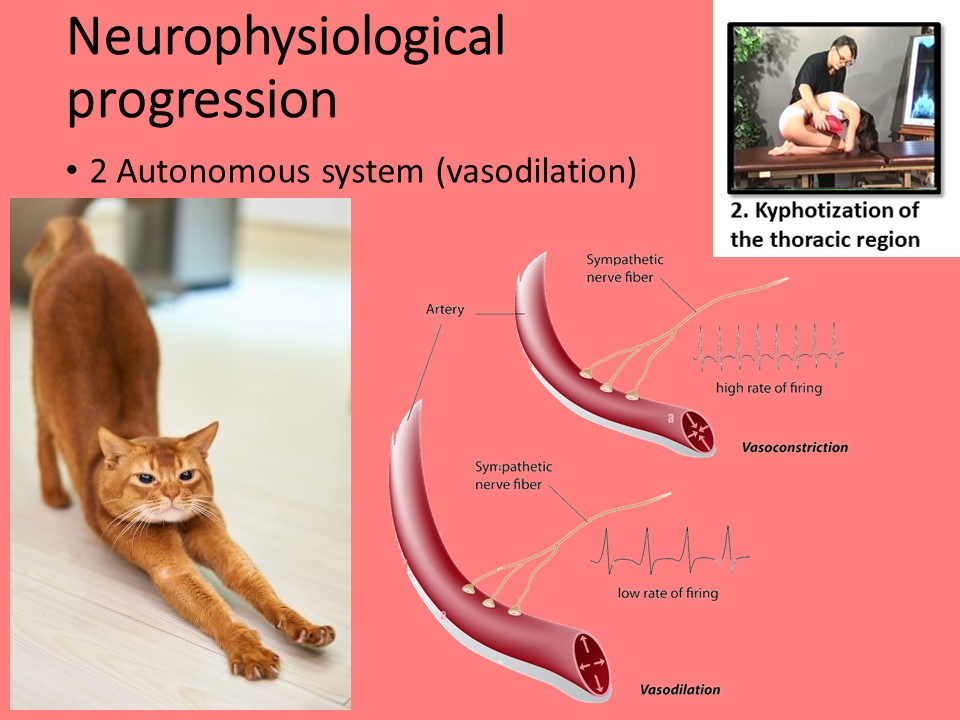 |
Stretching eliminates toxins and lactic acid accumulated through inactivity. It's a muscular awakening that's essential for further exercise. |
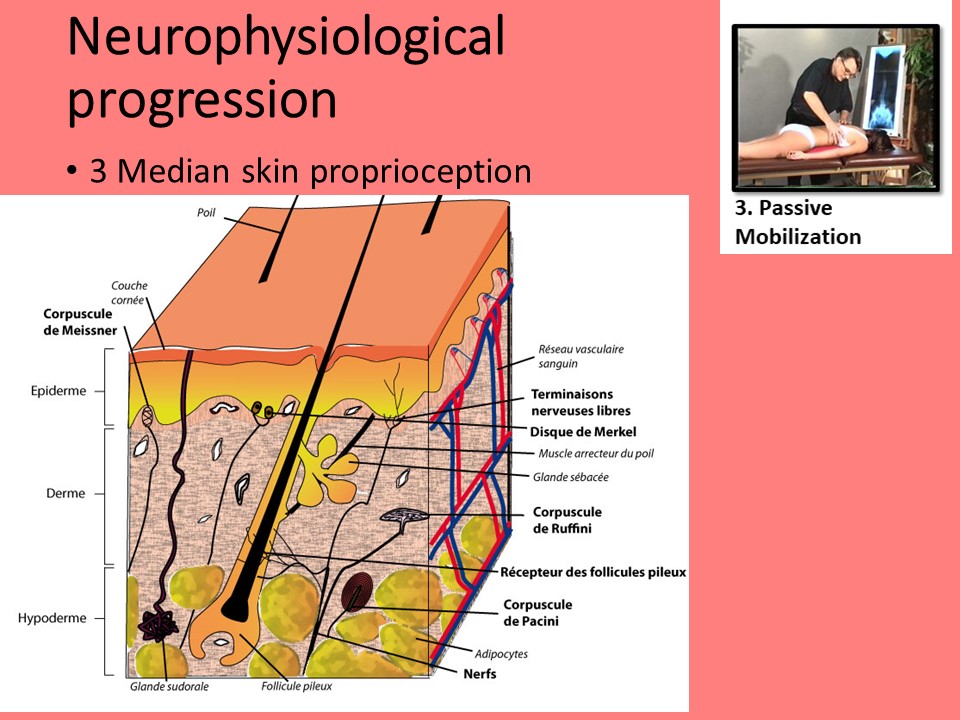 |
Proprioceptive stimulation of the skin involves Ruffini's and Pacini's corpuscles, which are very numerous along the midline. |
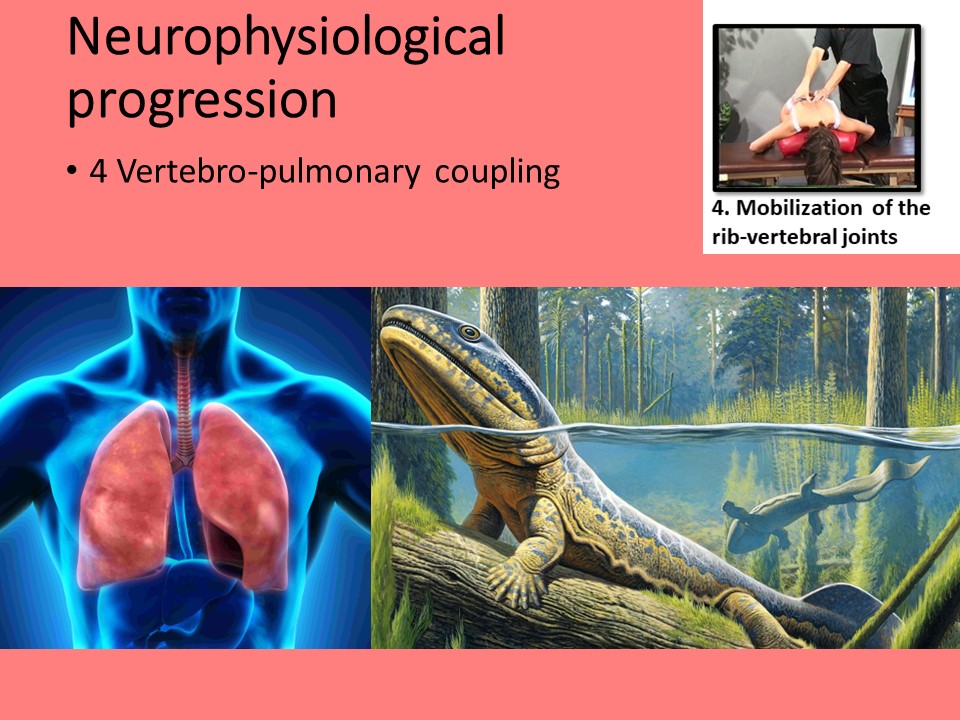 |
Vertebro-pulmonary coupling is fundamental when a child learns to swim, and later when practicing sports. The mobility of each segment is essential to vertebral tensegrity, particularly at the apex of scoliosis.
|
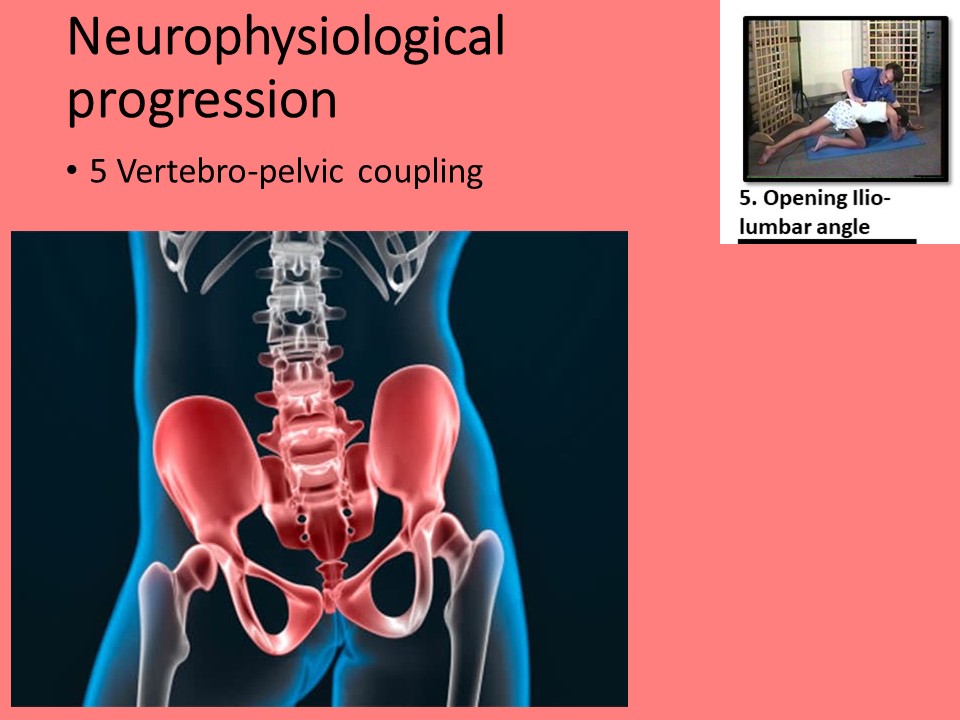 |
Realignment of the lumbopelvic spine with symmetrical tension of the iliolumbar ligaments is not dependent on growth plate and can be achieved at any age using the iliolumbar angle opening and the iliac plateau of the brace. |
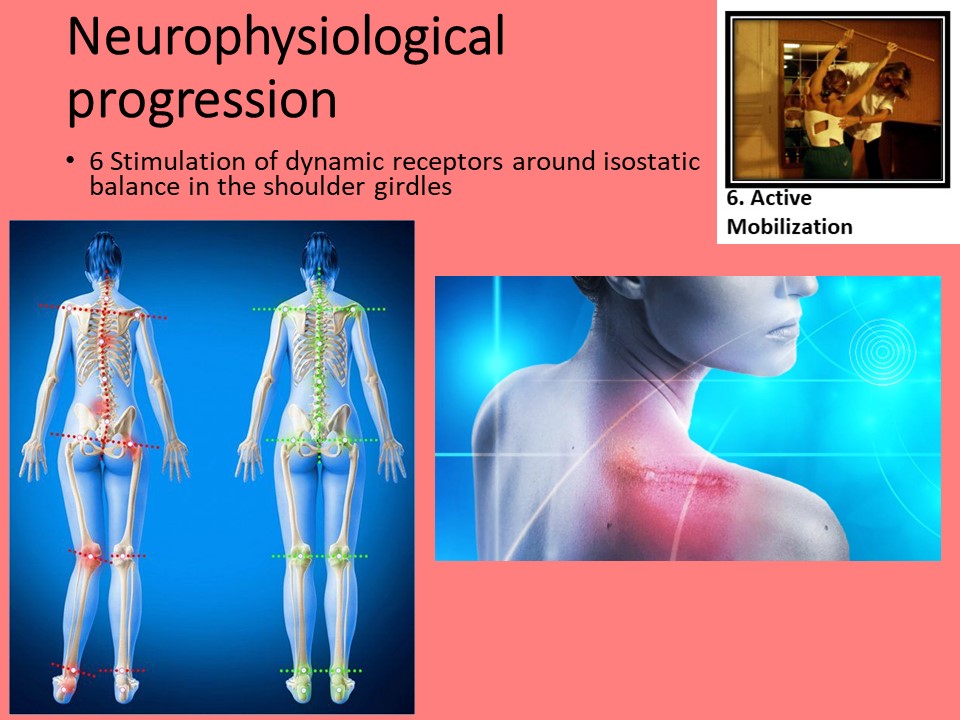 |
Imbalance of the shoulder girdle is often a compensation mechanism for scoliosis. The principle of the Lyon method, unlike Schroth, is to keep the receptors of the girdle, cervical spine and head in the vertebral axis. This means keeping the semicircular canals and the gaze in a horizontal plane. Scoliosis is therefore corrected below the shoulder girdle using the brace. |
 |
Once the girdles have been stabilized, the muscular receptors on either side of the vertebral axis will be called upon, all the more so as the correction of the curvature will be significant. |
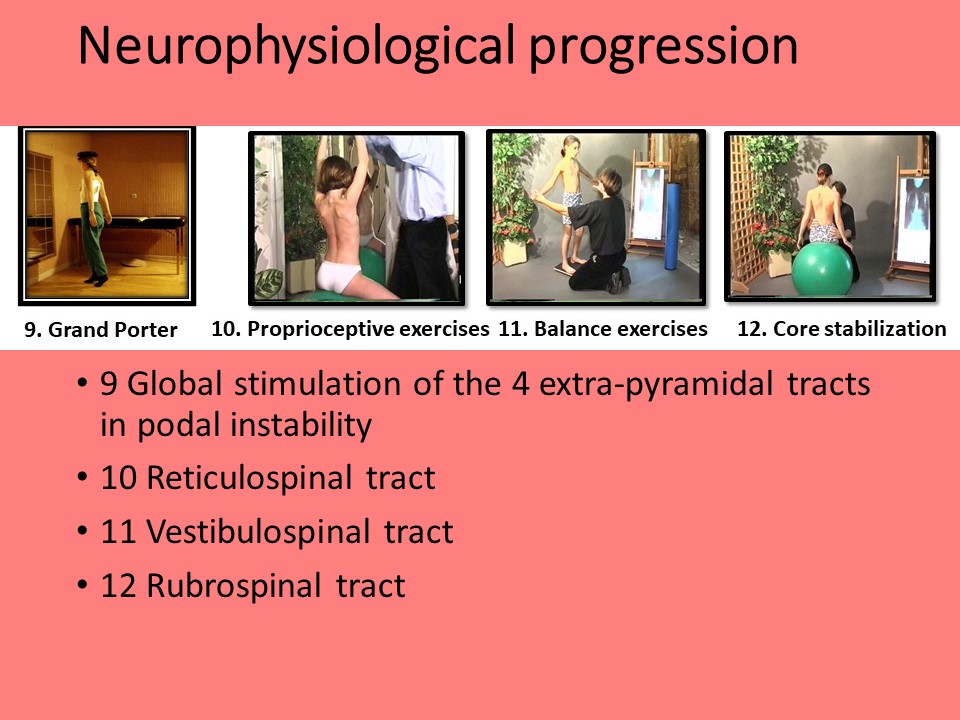 |
The last 4 exercises will specifically stimulate the 4 tracts of the extra-pyramidal system.
|
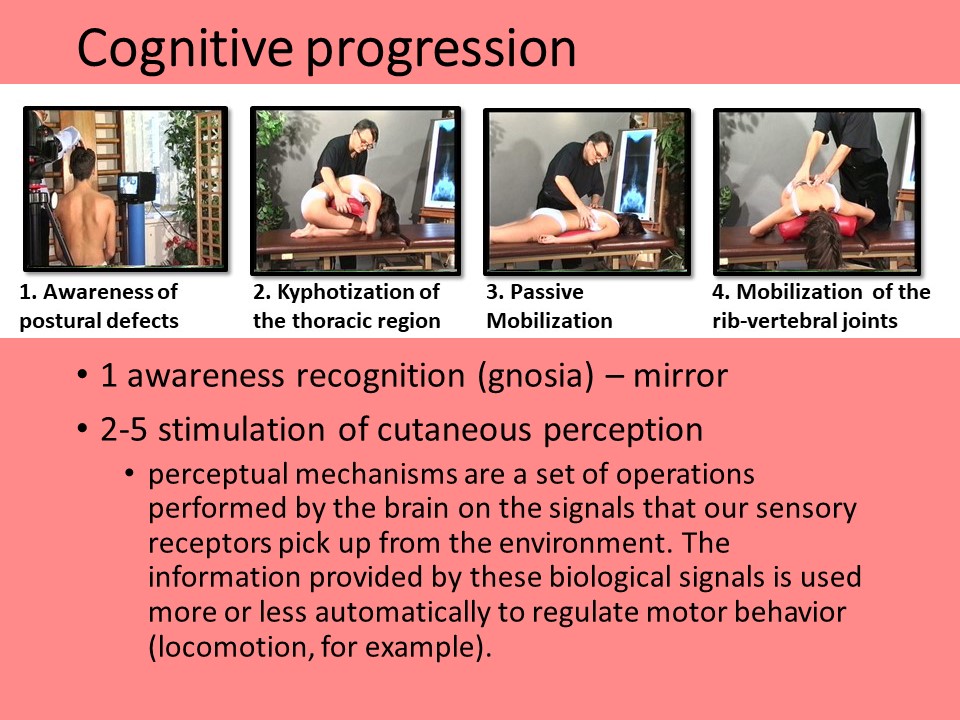 |
At the same time, there is a cognitive progression. The first exercise involves visual, auditory and digital gnosis. The physiotherapist must speak and touch the patient, correcting him or her. Exercises 2 to 5 stimulate skin perception receptors. Perceptual mechanisms are a set of operations performed by the brain on the signals that our sensory receptors pick up from the environment. The information provided by these biological signals is used more or less automatically to regulate motor behavior (locomotion, for example). |
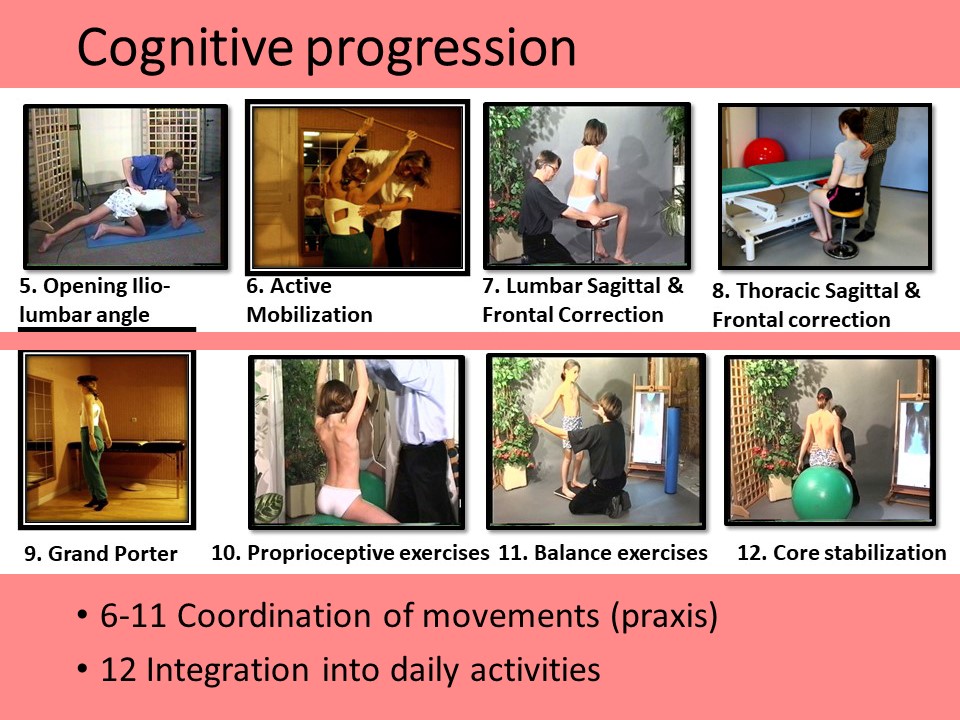 |
Exercises 6 to 11 stimulate praxis, that is, all the functions involved in coordinating and adapting basic voluntary movements, with the aim of successively correcting scoliosis region by region, then globally, maintaining the corrected position in situations of imbalance. The twelfth exercise reinforces the corrective praxis of deviation in all situations of daily life. |
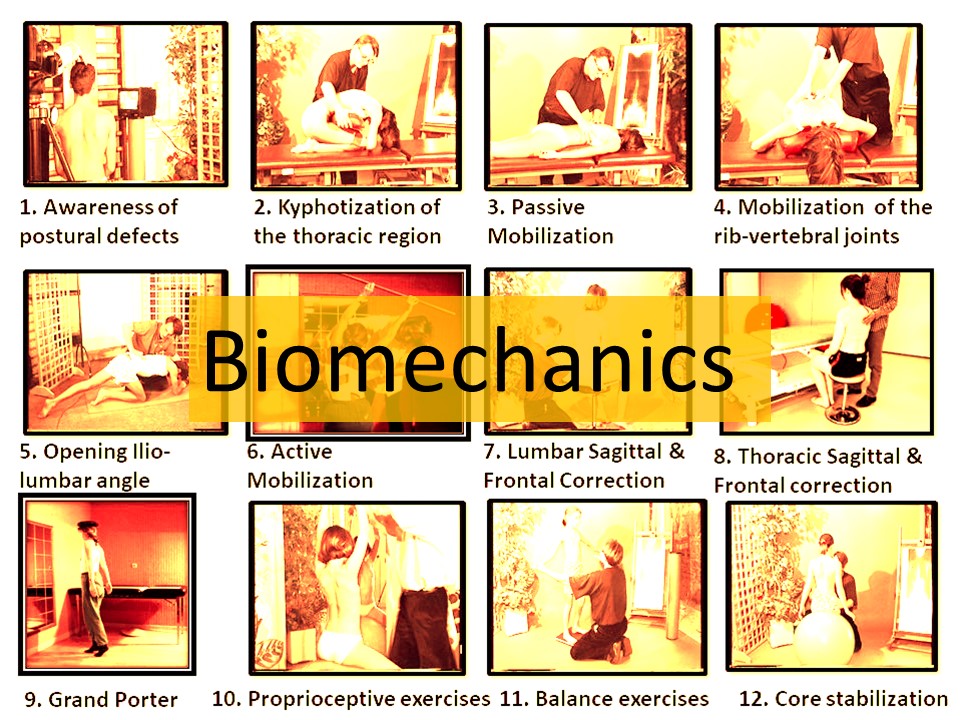 |
The Lyon method is the only one to combine a specific, complementary brace with physiotherapy. The 12 exercises are based on the same biomechanical principles for correcting scoliosis. |
 |
As virtual reality can improve sports performance, this first phase of physiotherapy allows the brain to integrate the corrected position. The correction will be carried out according to the principles of global detorsion.
|
 |
Stretching is used in many different ways. The benefits are manifold: it increases joint mobility and improves the condition of muscles, tendons, ligaments and connective tissue.It improves postural tone and relieves chronic back pain. Prevents muscle strains, sprains and tears. Stretching is anti-stress. It improves gestural coordination. |
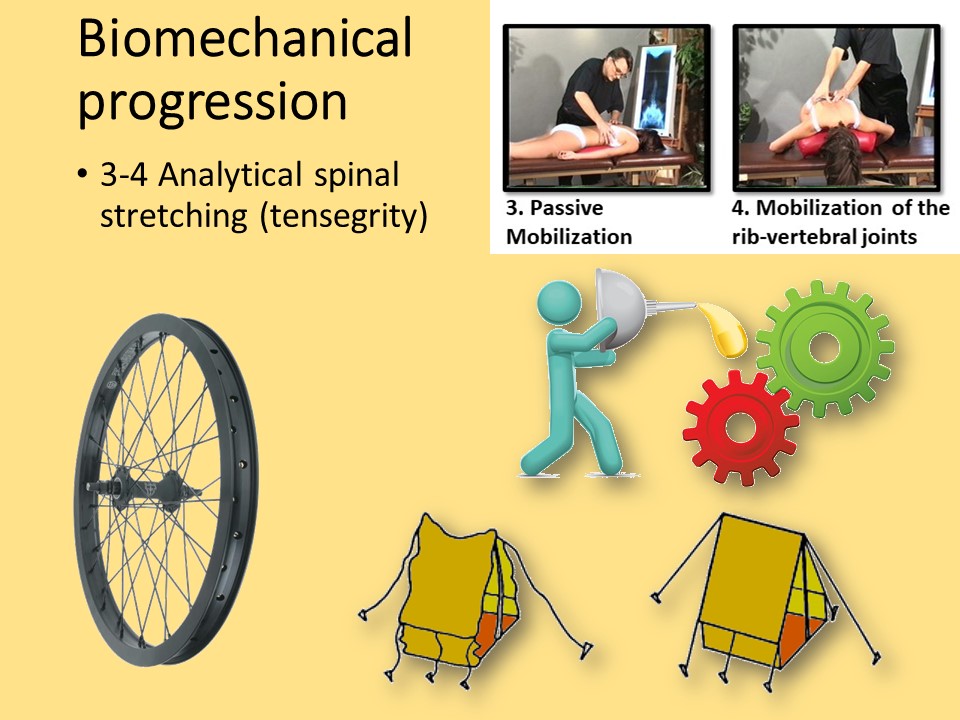 |
Scoliosis is accompanied by apical rigidity with mini-blocks and hypermobility at the ends of the curvature. Symmetrization of tensions is therefore necessary to obtain maximum tensegrity, a little like oil in vertebral cogs. |
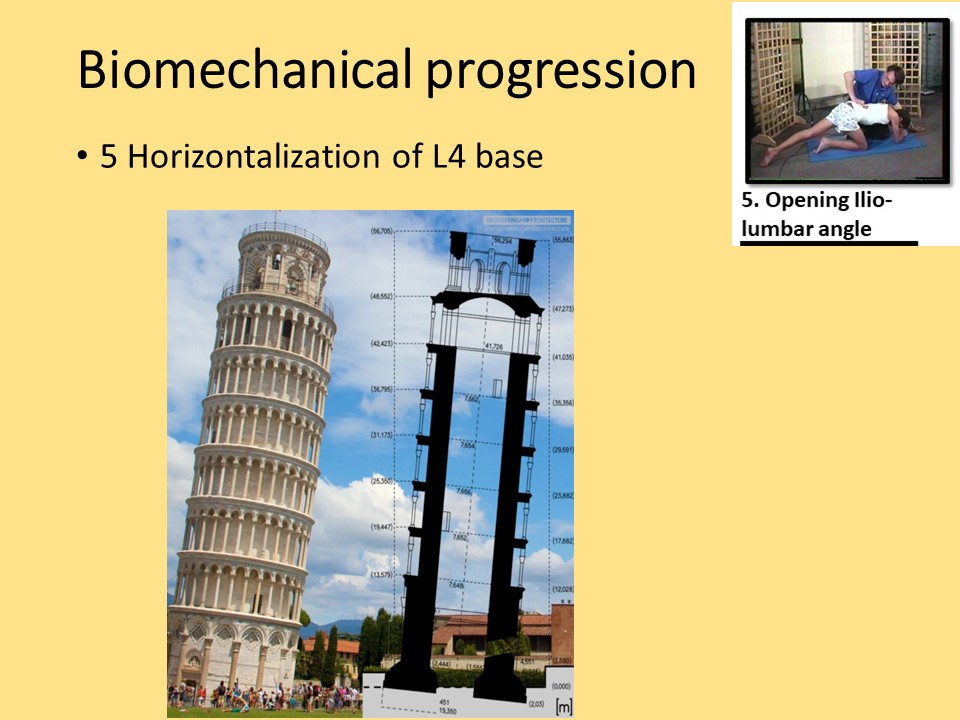 |
All construction requires a stable horizontal base. Correcting scoliosis by maintaining the oblique start will unbalance the occipital axis on the line of gravity. |
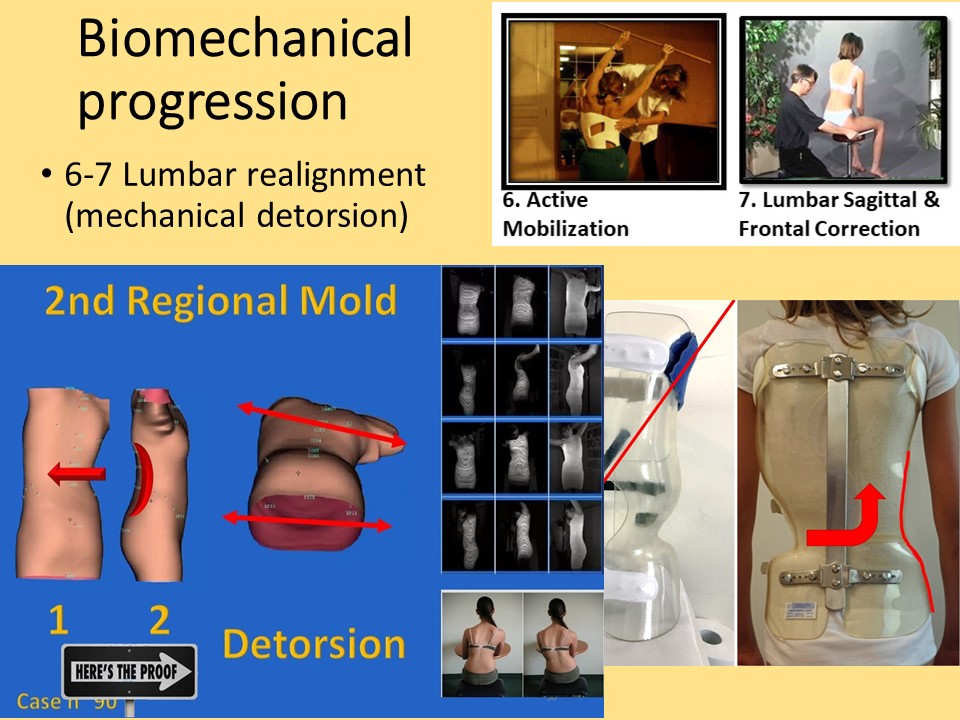 |
A particular feature of the Lyon method is the lumbar regional mechanical detorsion achieved by coupled movements in the sagittal and frontal planes. Unlike the Chêneau brace, there is no expansion in the concavity. Bumping up against the wall of the concavity, the only possibility for the soft tissues is to move upwards. This is the push-up effect.
|
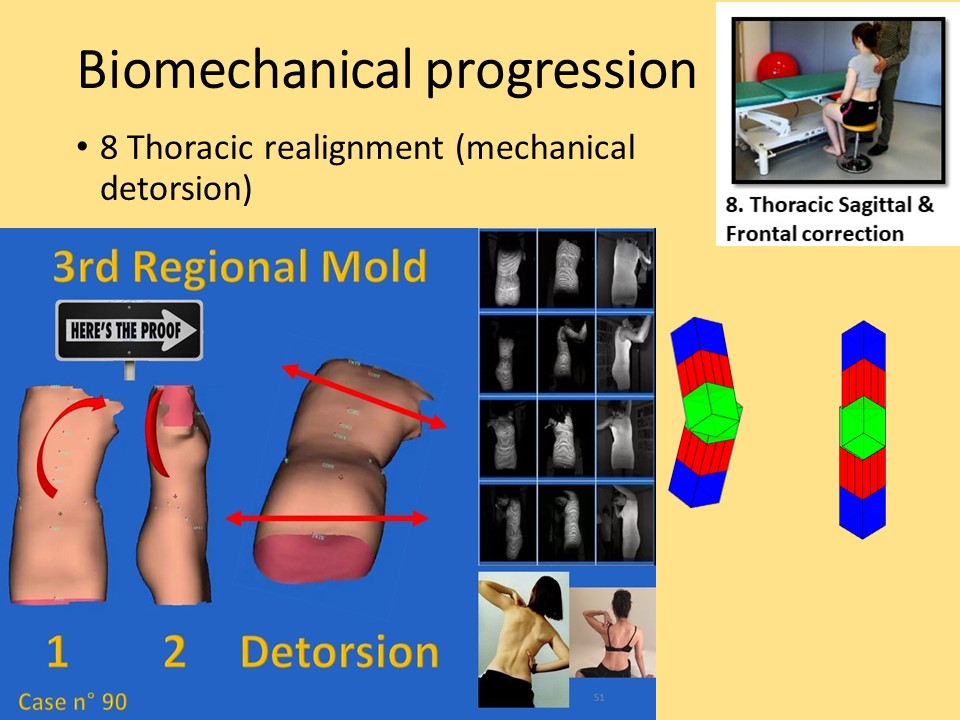 |
At thoracic level, bending is performed while keeping the shoulder girdle horizontal and centered on the line of gravity. Mechanical apical detorsion is only performed between two fixed points. |
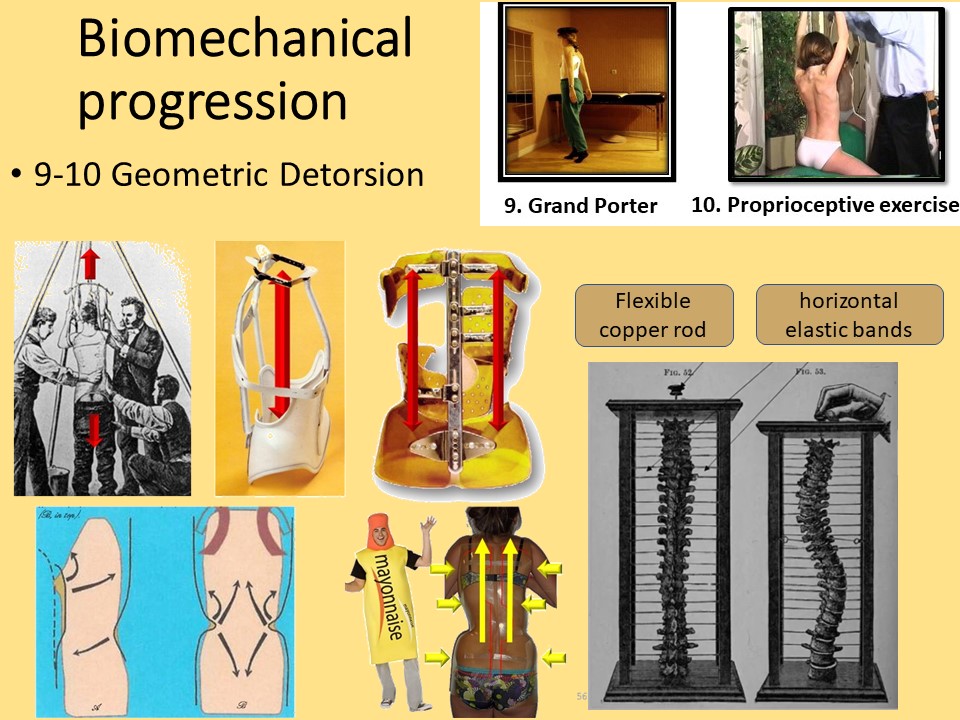 |
Geometric detorsion is one of the foundations of scoliosis correction. Lewis Sayre's experiment illustrates the buckling effect of scoliosis formation with correction by pulling vertically on the copper axis. In the Lyon method, this correction is aided by the effect of the mayonnaise tube. |
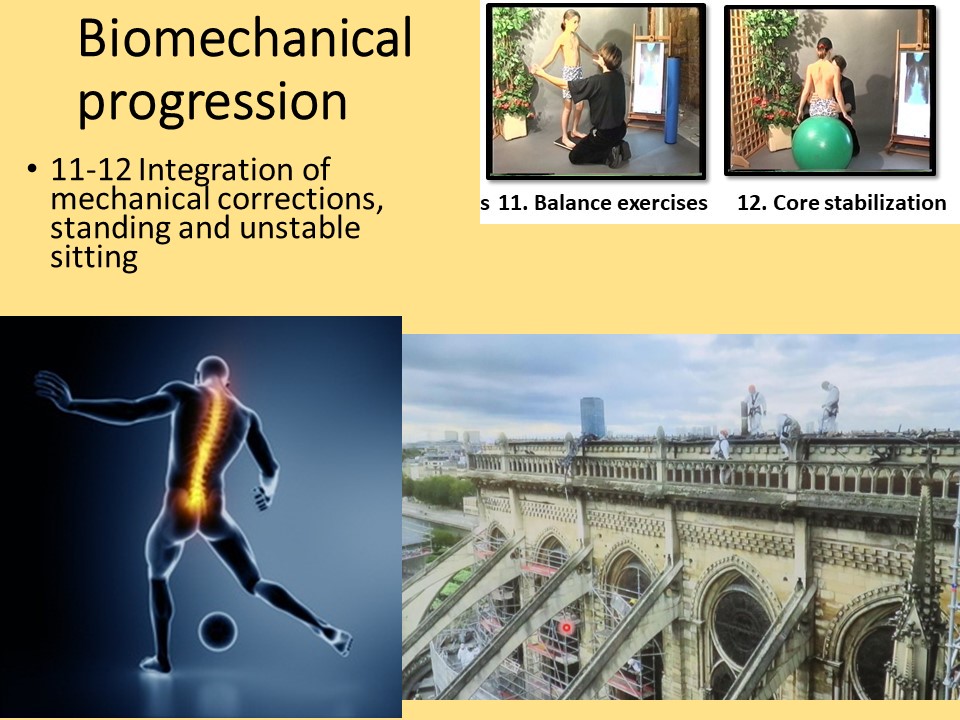 |
These corrections are maintained first statically, then dynamically, by gradually increasing the imbalance, while reinforcing the support structures. |
 |
Gravity is a fundamental element of biomechanics and epigenetics. If awareness is gained in an upright position, the following 4 exercises are performed lying on the examination table, then on the floor in a quadrupedal position like the Klapp.
|
 |
In the sitting position, the spine is vertical and isostatically balanced in the sagittal plane. The sitting position will be modified, from stable to unstable |
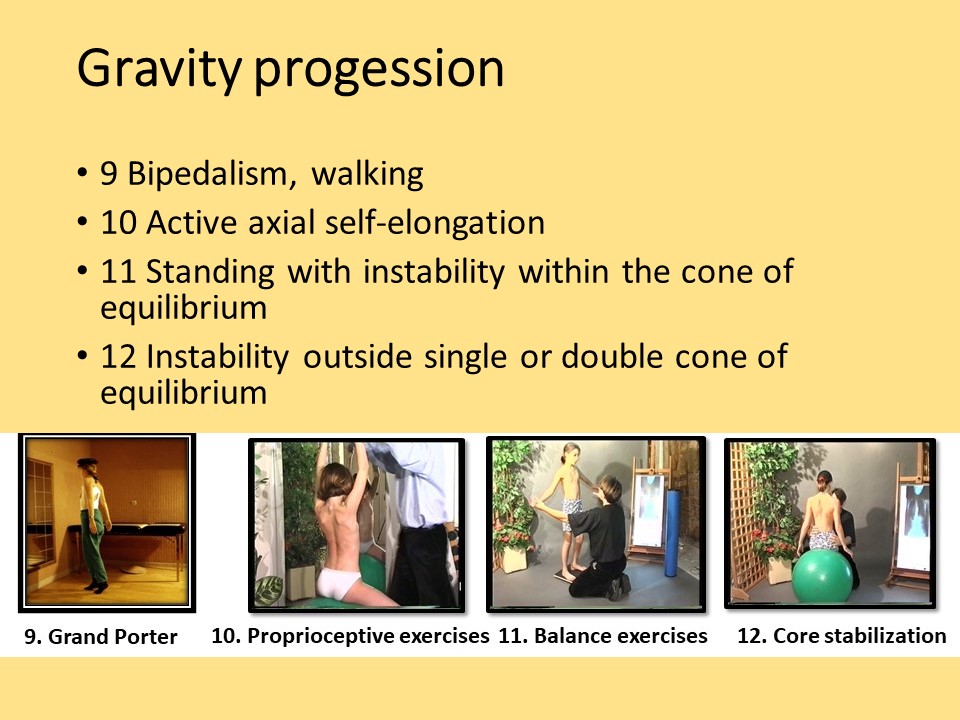 |
Exercises 9 to 12 are performed in an unstable standing position. Instability is either podal or pelvic on a Swiss ball. Exercise 12 is performed in all positions, with the kinetic chain closed and then open.
|
 |
As the treatment progresses, there is a temporal progression, usually in the fourth dimension. Once the patient is aware of the deviation, the spine is softened as a whole. Corrections are then made upwards from the lumbosacral hinge to the thoracic region. If angulation exceeds 20°, a brace is applied to help maintain the corrected position. This corrected position must be maintained in an unstable position, which requires specific strengthening of the core muscles. |
 |
In conclusion, the 12 basic exercises of the Lyon method cover most of the components of scoliosis physiotherapy in a logical progression. All exercises are performed in low-resistance aerobic metabolism, in individual sessions of 35 minutes + 5 minutes back training. Daily repetition of a 10-minute home exercise improves epigenetic efficiency. All other epigenetic components are also taken into account: hydration and nutrition, channelling of sports practice. The patient must enjoy the exercise, which relaxes both body and mind. Networking is facilitated by the online support of the Lyon method.
|