Twelve particular cases of scoliosis
It is distressing to think that such a large deformity can appear in an otherwise healthy child, and that we still have no idea where it comes from.
JIP James, surgeon
 |
It is customary to take the simple right thoracic and/or left lumbar scoliosis as the type of description. The advantage is didactic and pedagogical with simplification. In the daily reality, 12 particular clinical situations can be identified and sometimes associated. |
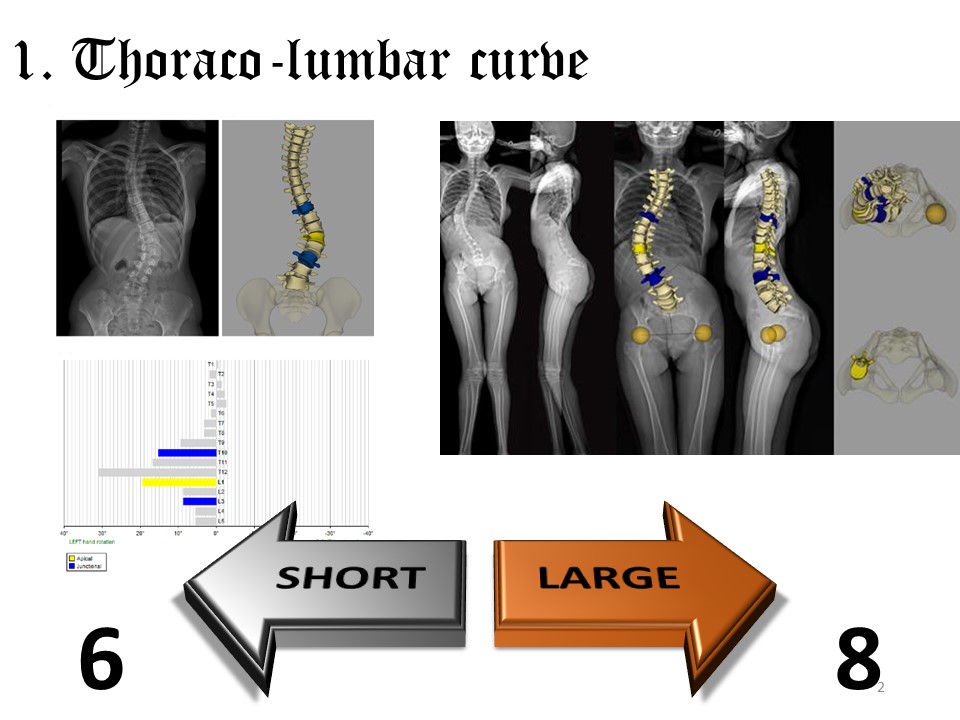 |
The first special case concerns thoracolumbar scoliosis with apical vertebrae at the thoracolumbar hinge level. Contrary to the thoracic and lumbar curvatures whose rotation by coupled movements is explained by the anterior cuneiformization of the vertebral body at the thoracic level and posterior cuneiformization at the lumbar level, the thoraco-lumbar rotation thus seems primitive. Given the frequency of this type of curvature in de novo scoliosis, a displacement of the nucleus of the intervertebral disc or a musculo-ligamentary asymmetry is logical in adolescents. The thoraco-lumbar curve can be short with 6 vertebrae included in the curve or larger with 8 or more vertebrae like neurological scoliosis. |
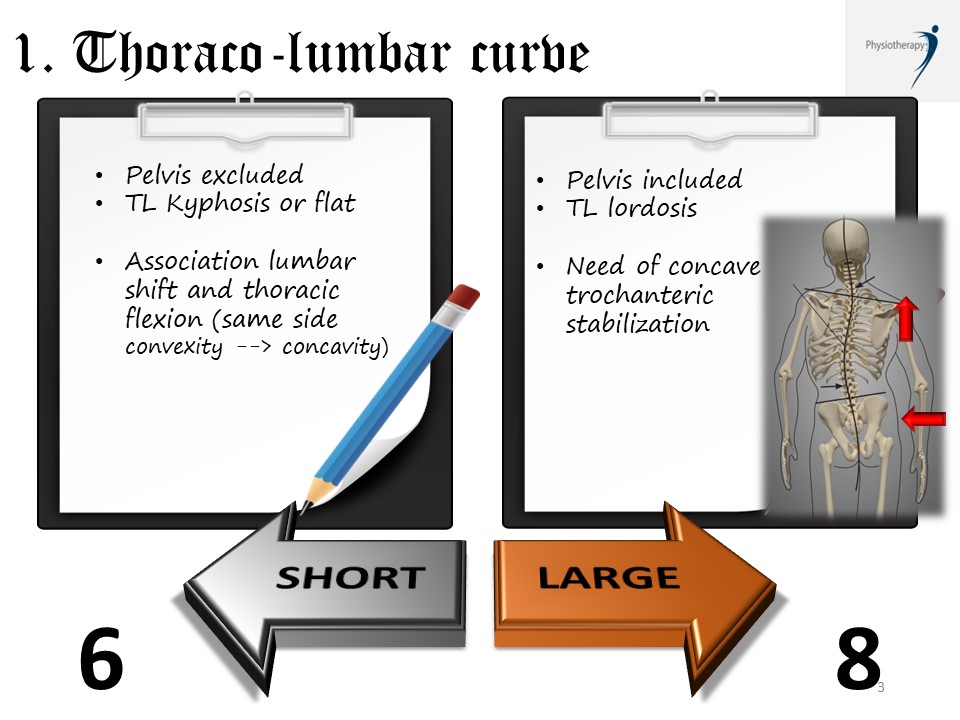 |
The short curve of probable disc origin is often associated with an excluded pelvis with a tendency to thoracolumbar kyphosis. Physiotherapeutic correction must ensure control of the sagittal plane, especially in cases of low pelvic incidence. In the frontal plane, the corrective movement combines a lumbar shift and a thoracic bending centered on the thoracolumbar hinge and carried out from convexity to concavity with coordination of both thoracic and lumbar regions. The large curvature of probable musculo-ligamentary origin is often associated with an included pelvis. Physiotherapeutic correction is performed between the scapular girdle and the pelvic girdle, which is stabilized at the concave level. |
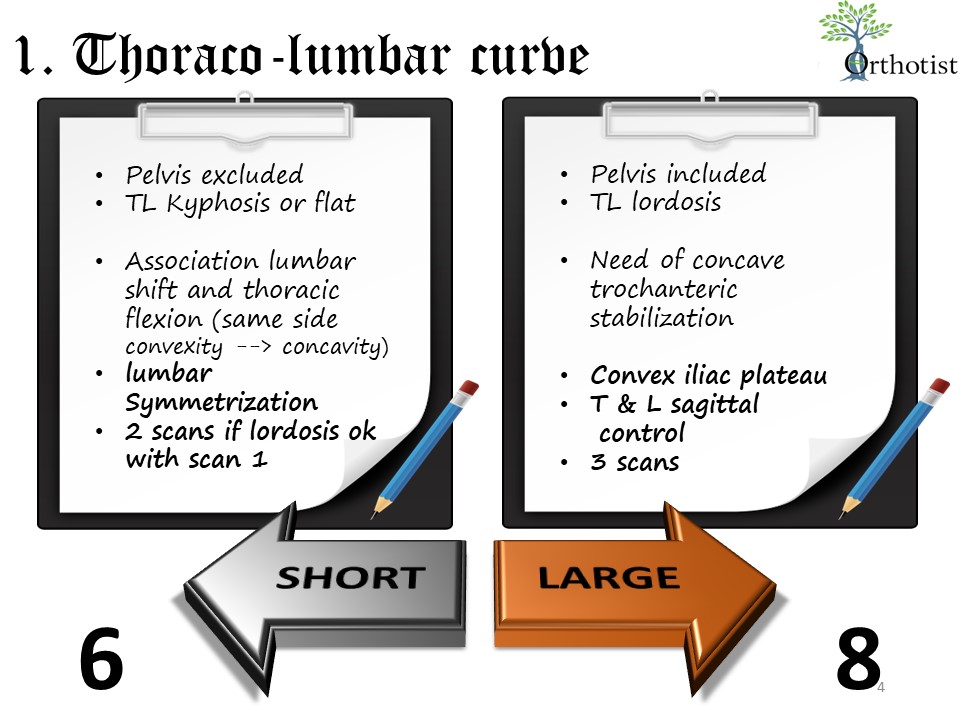 |
For short curves, when the brace is necessary, the thoracic and lumbar scans in the frontal plane will be performed in the same direction. The iliac crests will be symmetrized without an iliac plateau. In the sagittal plane, if the lumbar lordosis is well stabilized on scan 1, only scan 3 will be performed stabilizing the thoracic kyphosis. Often an additional metallic hinge at the thoraco-lumbar level will be useful to avoid any deformity in the sitting position. Hyper-corrective night braces are very effective for this type of curvature. For large curvatures, the concave pelvis is stabilized manually with lowering of the concave iliac crest, the convex iliac plateau remains moderate. The 3 scans are necessary with control of both pelvic and scapular girdles. An elevation of the concave shoulder is performed in case of initial imbalance. Plastic deformation with initial full time is very effective for this type of curvature. |
 |
In case of a long thoracic-lumbar curve, the use of a short GTB brace is possible, as there is less risk of creating a high thoracic counter-curvature. However, the sagittal plane is less well controlled in a short brace.
|
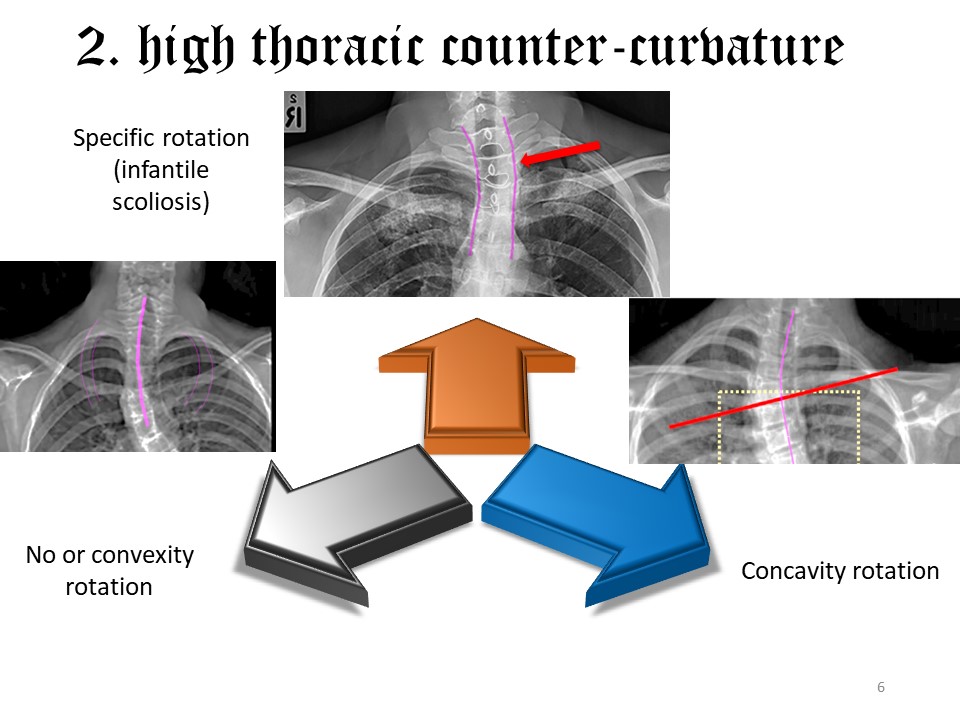 |
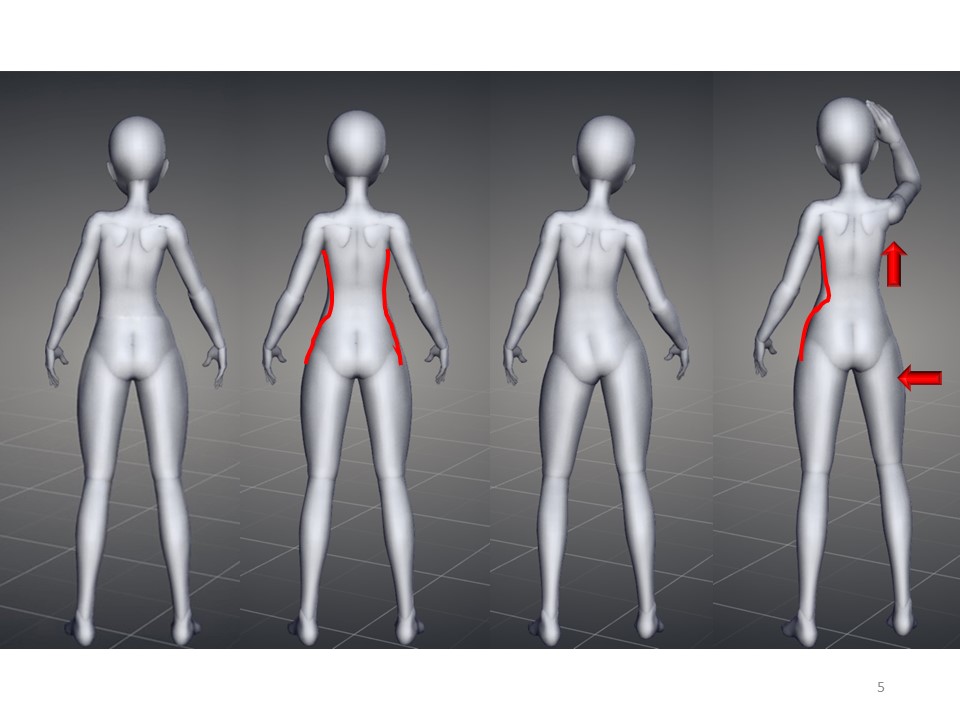
At the cervicothoracic junction, as at the thoracolumbar level, rotation seems more significant than frontal deviation. The high thoracic counter-curvature is a frequent and difficult case to control with underarm braces. Their evolution is generally slowed down by the scapular girdle. There is a special case of infantile scoliosis with specific rotation limited to T1. It corresponds to a locking that can favor the underlying deviation. For the other curves, it will be necessary to appreciate the rotation. |
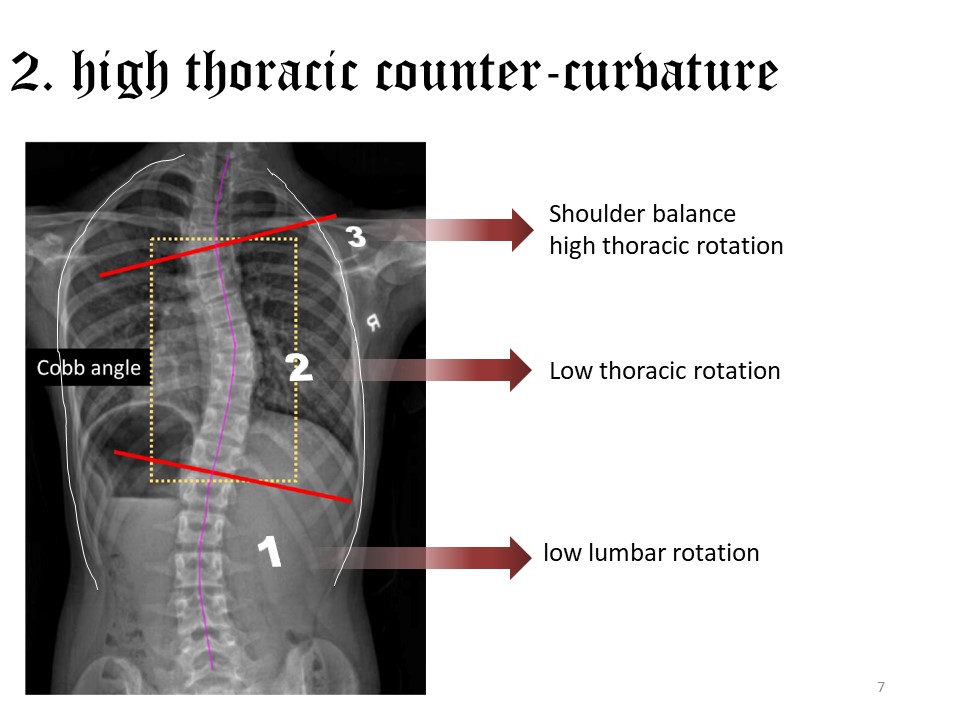 |
When there is a rotation, this counter curve can be considered as structural compensating the underlying rotations. The shoulders remain balanced. |
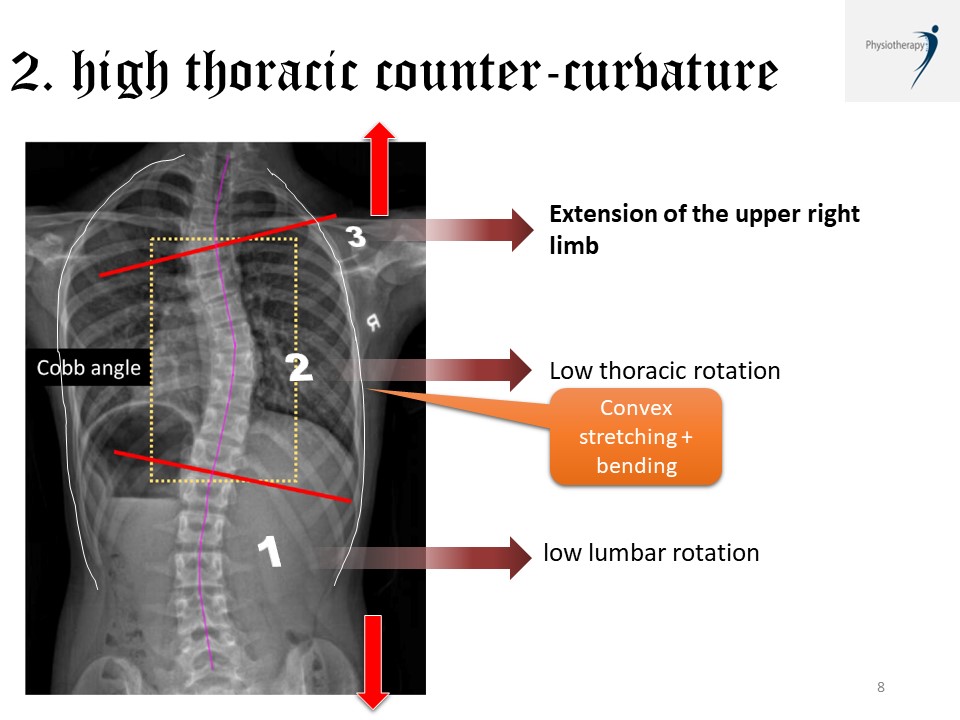 |
Physiotherapy will focus on global geometrical detorsion between the two girdles with global stretching of the thoracic convexity, which should be associated with corrective bending in the frontal plane. |
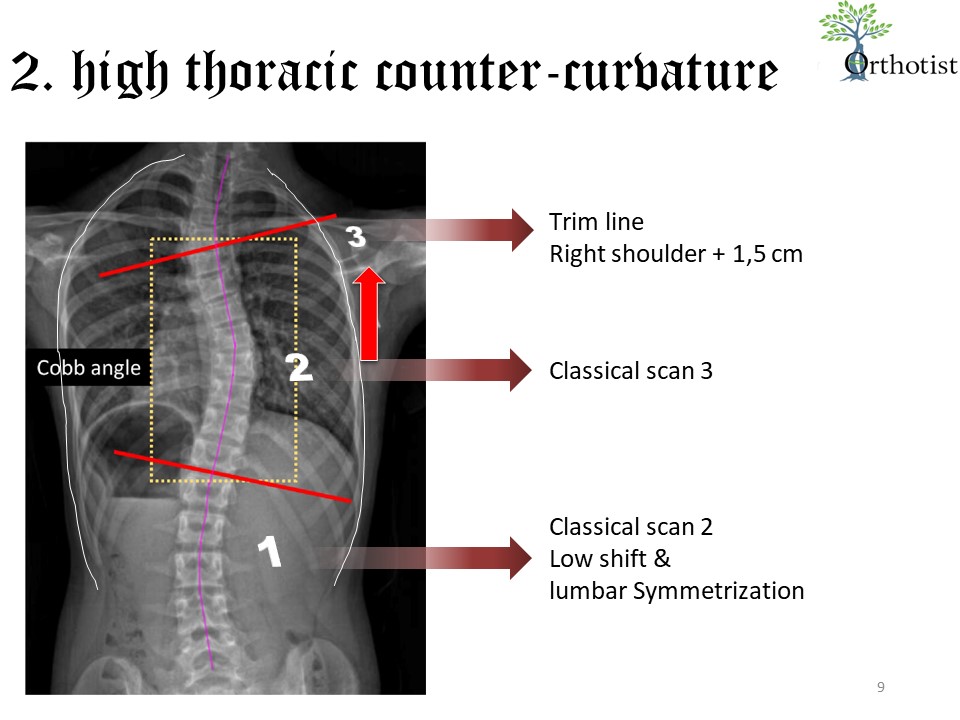 |
For the realization of the brace, scan 3 corrects the main thoracic curve normally. We can asymmetrize the high trim lines with +1.5 cm on the right. At the lumbar level, if the rotation is low, symmetrization is sufficient without iliac plateau.
|
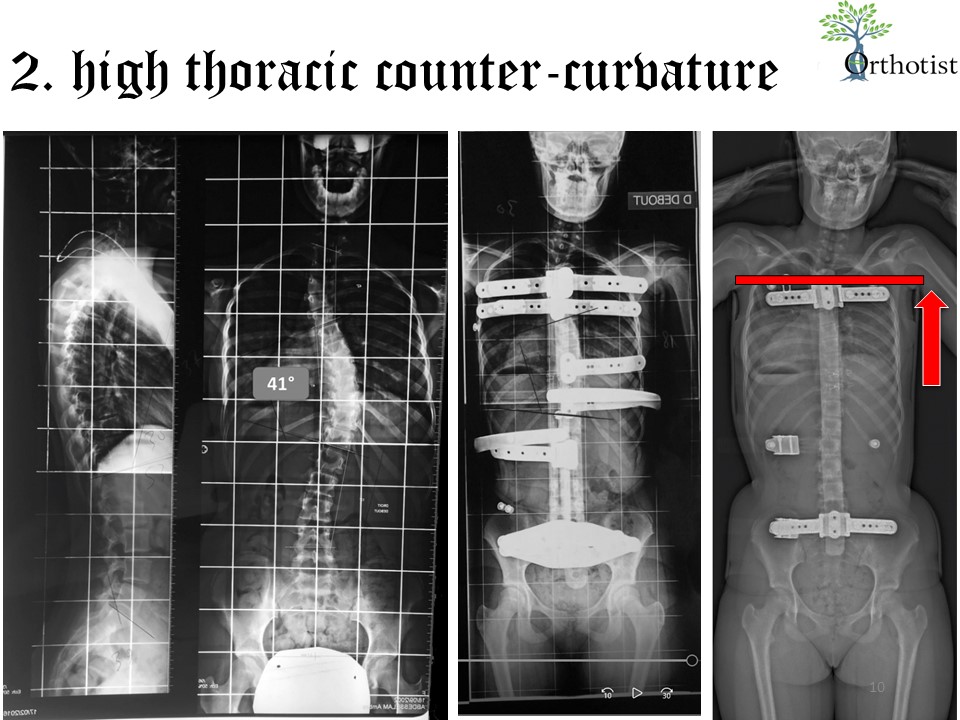 |
The high thoracic counter curve was less well corrected with the old Stagnara brace. The elevation of the right shoulder provides a better correction in ARTbrace. |
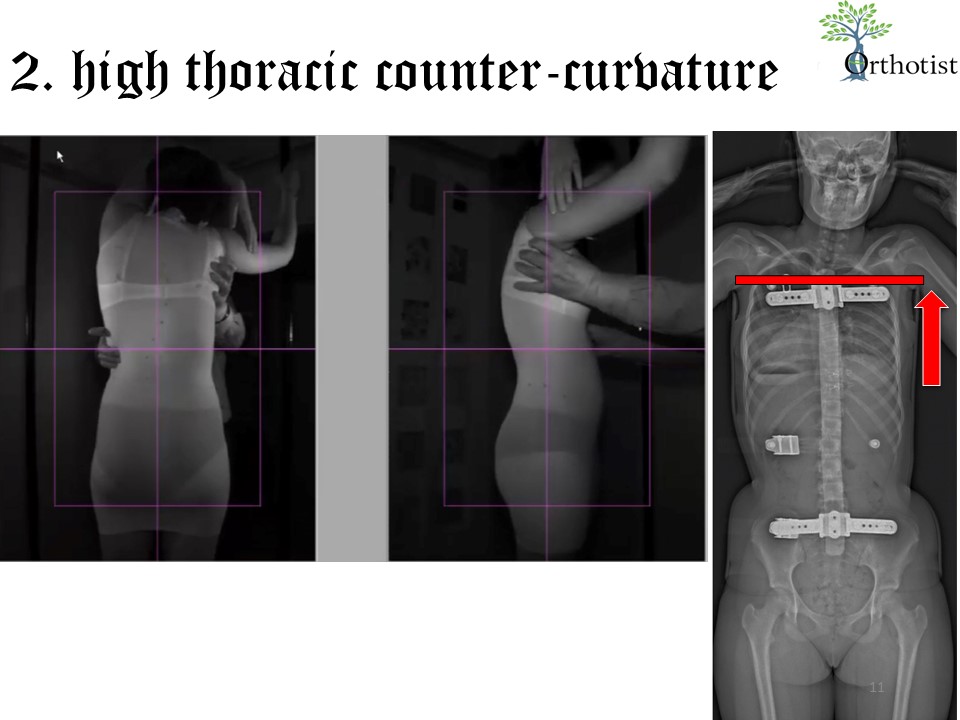 |
When performing scan 3, the right shoulder can be elevated. |
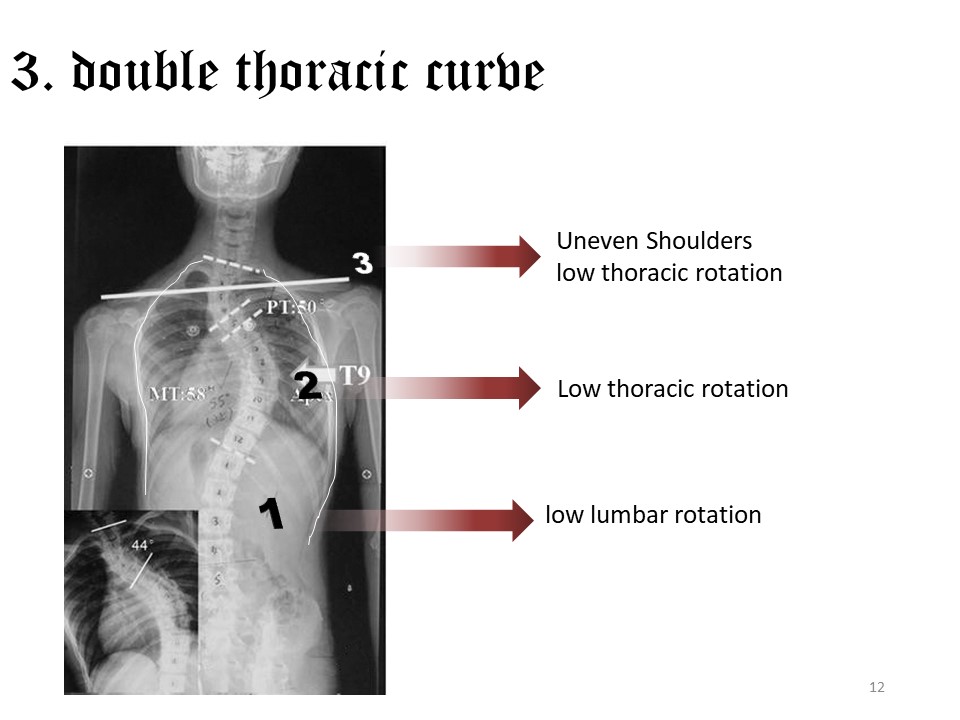 |
When the two thoracic angulations are equivalent, it is called double thoracic scoliosis. For infantile scoliosis, the specific rotation can be the cause of a double thoracic scoliosis. In other cases, it is the evolution of a high thoracic counter curve. The shoulders are often uneven and as before, the thoracic rotation is reduced. |
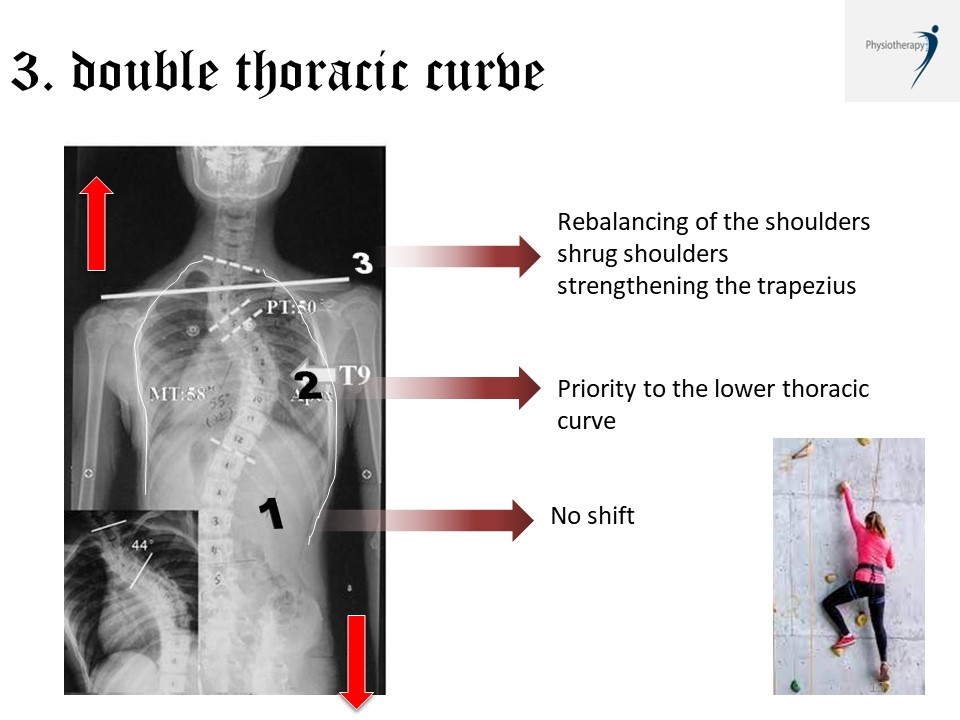 |
Priority is given to the lower thoracic curve, which is often more extensive. The extension of the left upper limb can therefore go in the direction of aggravating the upper curve. The trapezius here on the right will be strengthened to rebalance the scapular girdle. Climbing on the wall is especially recommended.
|
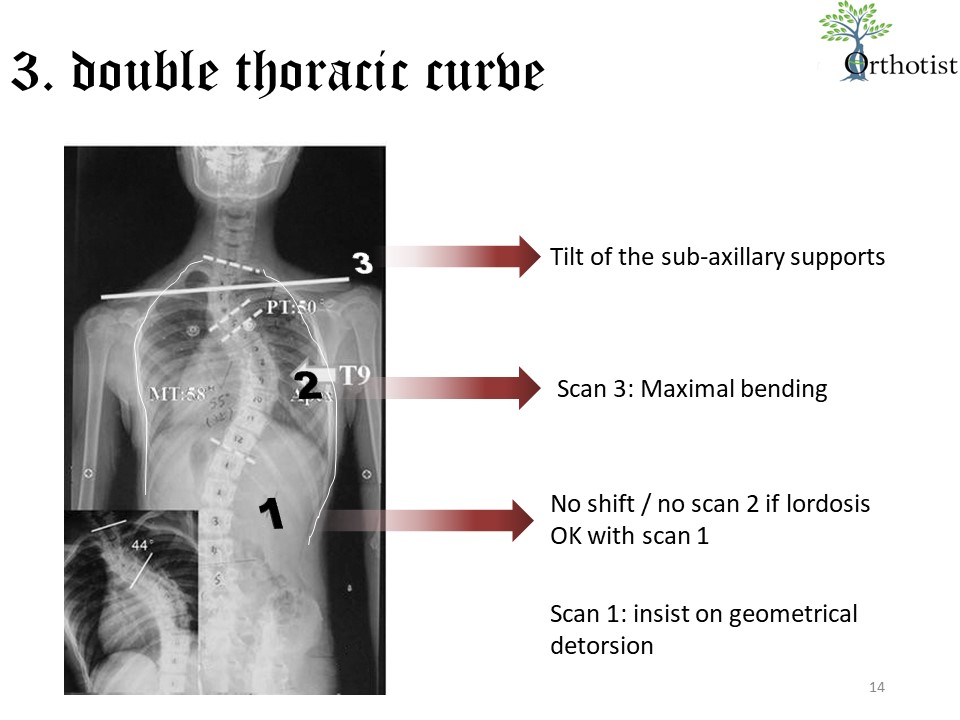 |
For the realization of the brace, the scan 3 corrects the lower thoracic curve. Technically, it is possible to perform a 4th scan by reversing the correction at the shoulder level. We insist on geometrical detorsion. |
 |
The lateral subaxillary supports are usually vertical. It is also possible to perform a thoracic bending of the upper thoracic region during processing, which will result in a tilt to the vertical of the subaxillary supports. |
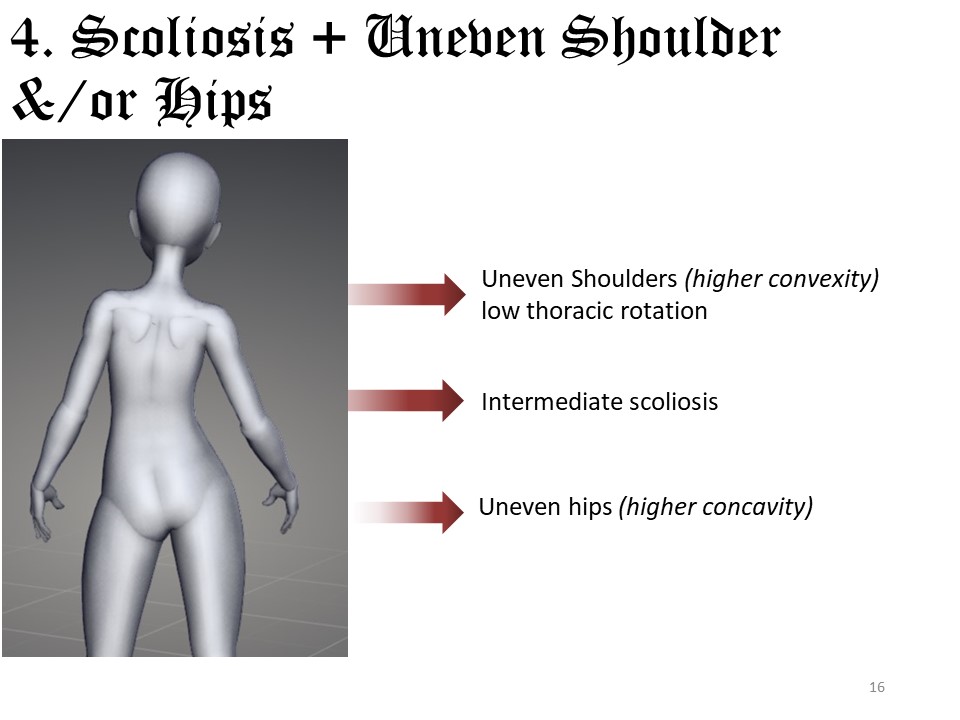 |
The shoulders and pelvis are non-deformable areas at the base of the thoracic and lumbar hyperboloids that allow detorsion. They can be rebalanced and reoriented. Shoulder imbalance with convexity elevation should be treated at the same time as the scoliotic curve, as we have seen for large thoracolumbar curves. |
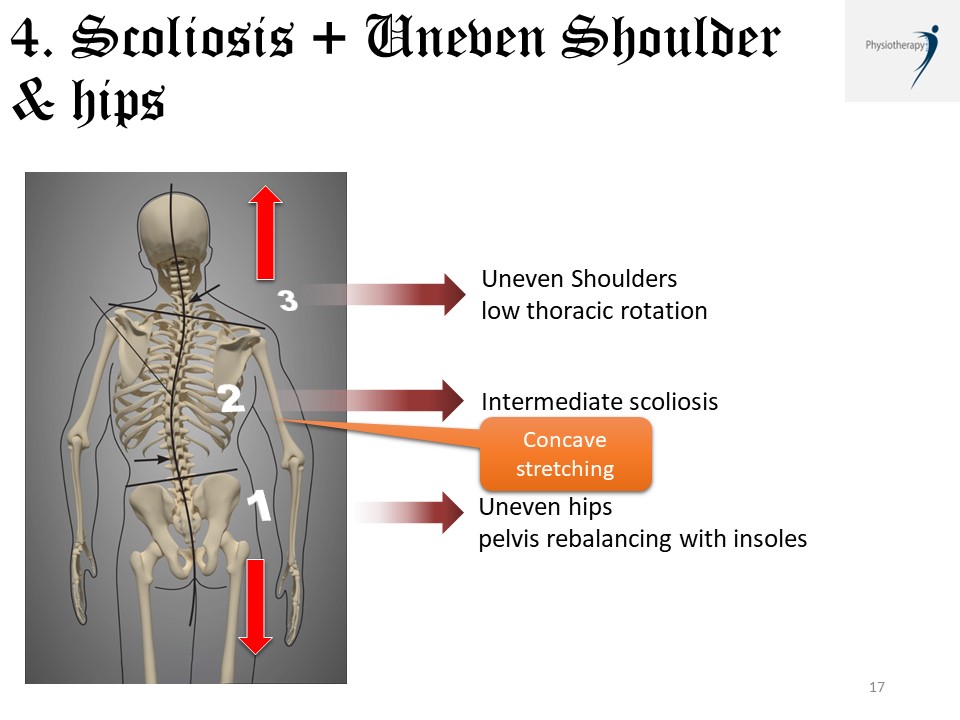 |
In this case, the first step is to rebalance the pelvis as in functional scoliosis. The correction of the scoliotic curve goes hand in hand with the rebalancing of the shoulders.
|
 |
The realization of the brace will follow the same logic with rebalancing of the pelvis for all the scans and a higher concave subaxillary trim line. |
 |
Sometimes it is the concave shoulder that is elevated. The imbalance of the shoulders is then a compensation and does not require any particular correction. |
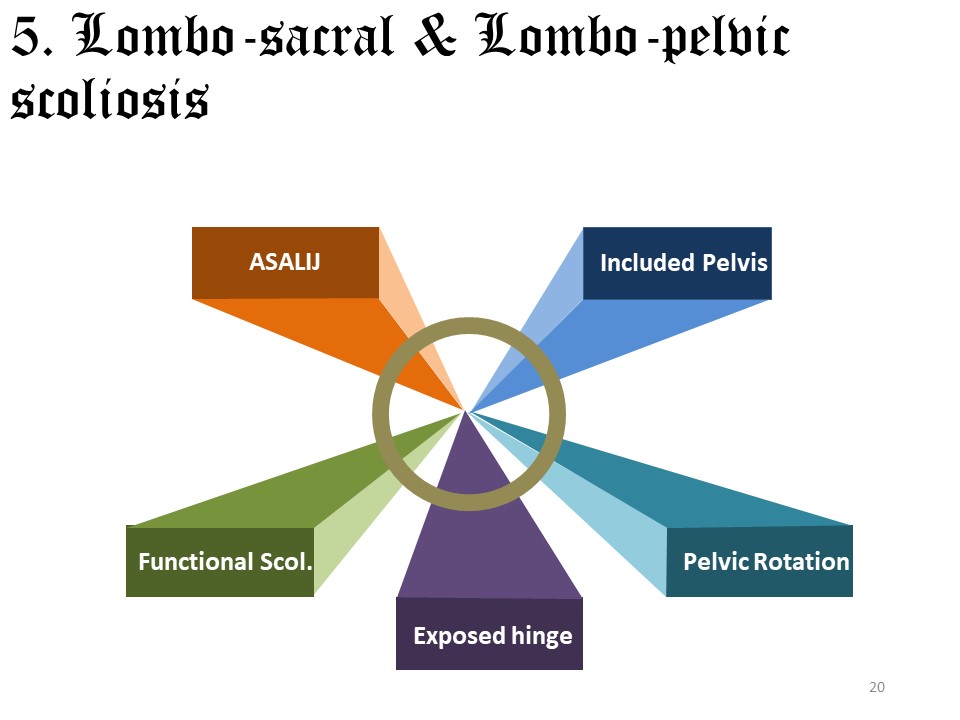 |
The Lyon Method takes into account lumbosacral and pelvic scoliosis. It will be necessary to differentiate: the Asymmetric Structural Anomaly of the Lumbo-Iliac Junction, the included pelvis, the pelvic rotation, the exposed hinge and the functional scoliosis. |
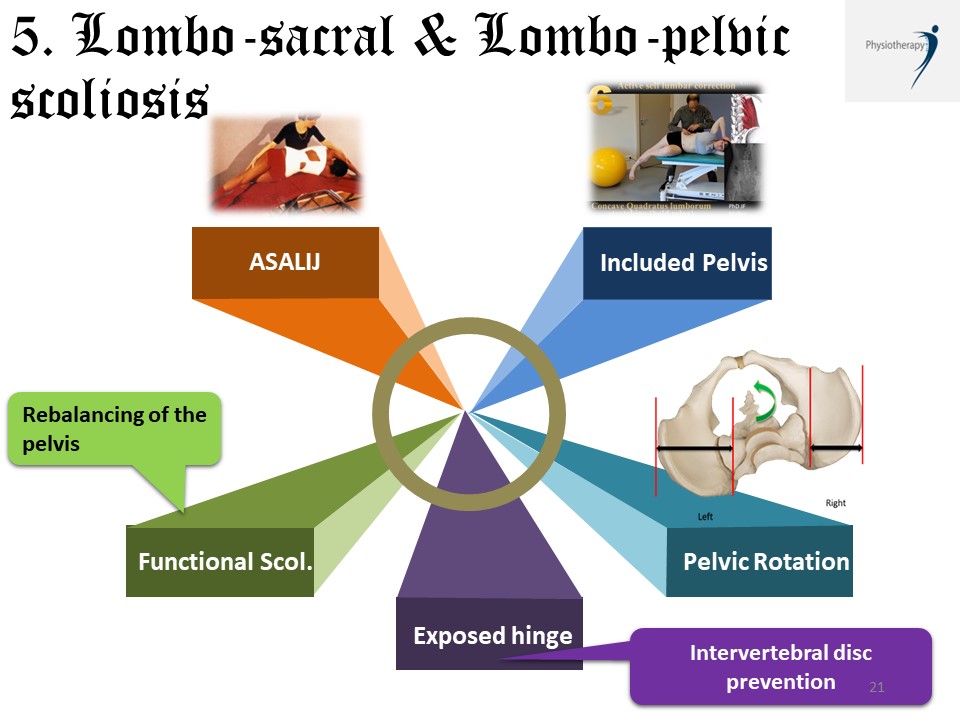 |
The indications will be specific: 1. Opening of the ilio-lumbar angle in case of tilt of L4, 2. Stretching of the lumbar concavity in case of included pelvis, 3. Pelvic rotation toward the concavity can be corrected by extending the concave hip relative to the opposite hip, 4. In case of an exposed hinge, prevention of disc degeneration should be emphasized, 5. In case of functional scoliosis, compensation of the unevenness is essential.
|
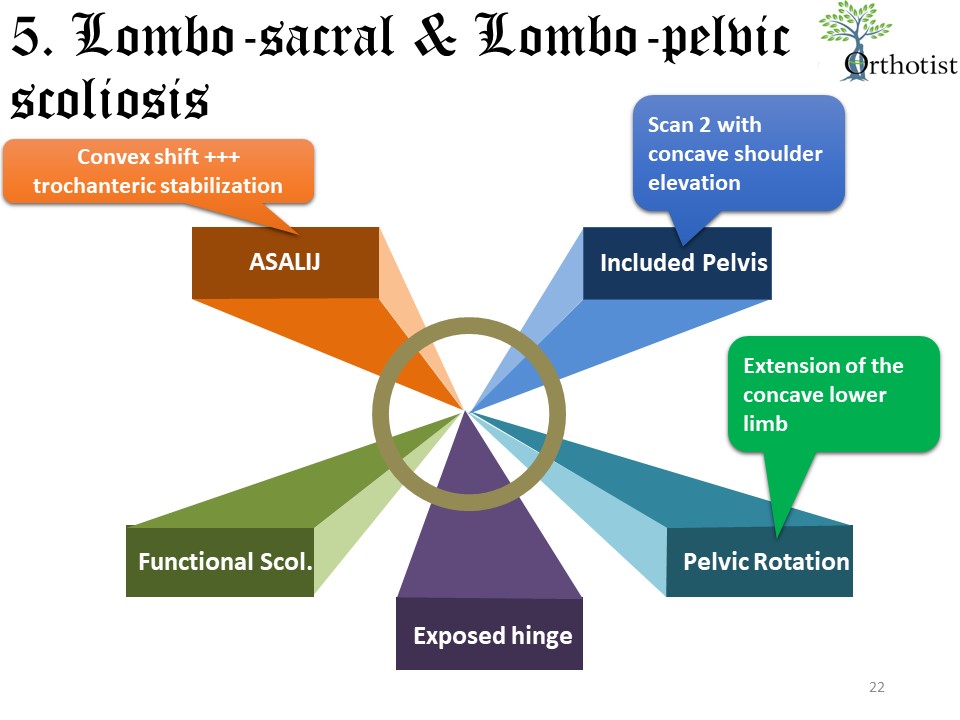 |
The same applies to the making of the brace: 1. Maximum convex iliac plateau with concave trochanteric stabilization in case of L4 tilt, 2. Scan 2 with concave shoulder elevation in case of included pelvis, 3. Pelvic rotation to concavity can be corrected by extension of the concave hip relative to the opposite hip in scans 1 and 2, 4. In case of an exposed hinge, no specific procedure is required, but prevention of disc degeneration should be emphasized, 5. No brace in case of functional scoliosis. |
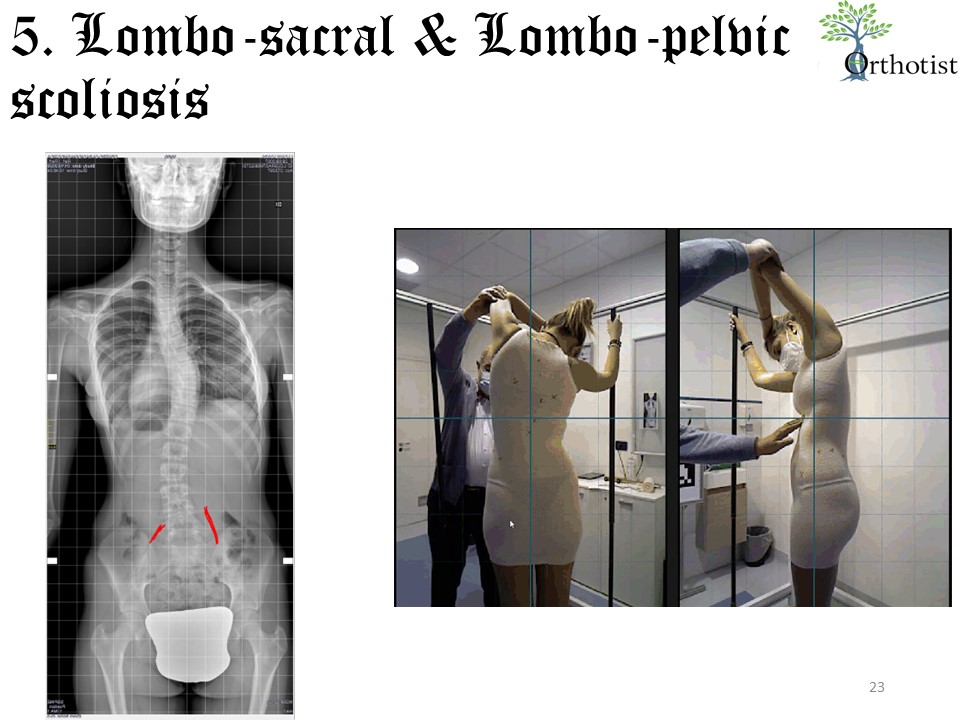 |
In this example of thoracic scoliosis with L4 tilt, the ilio-lumbar asymmetry draws the pelvis to the side of the shorter ligament on the convexity and also requires manual trochanteric stabilization. |
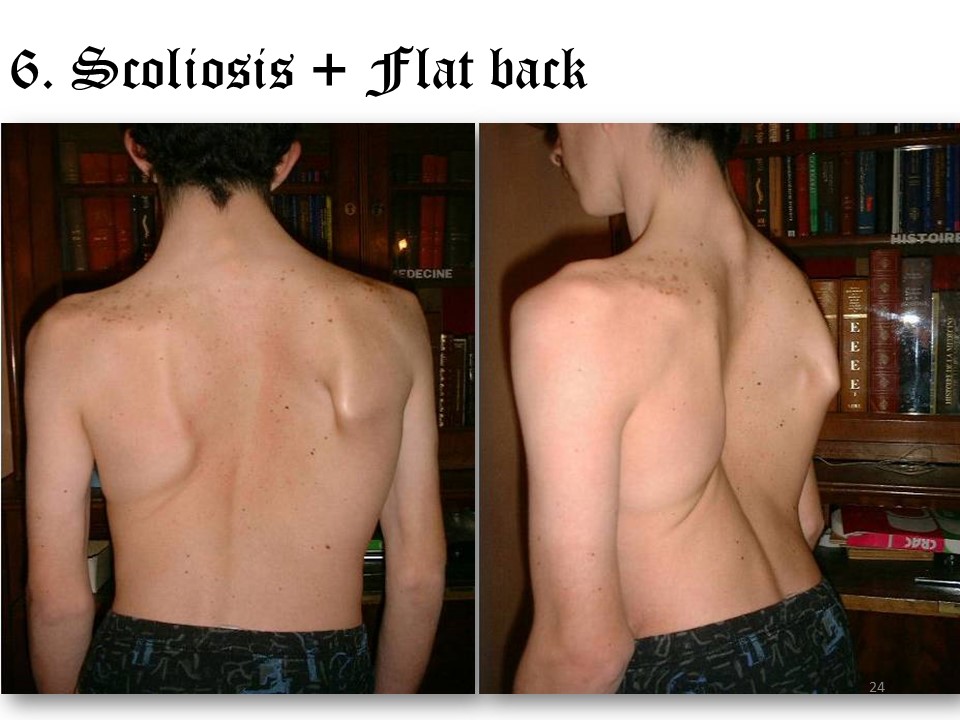 |
Half of the scolioses of adolescence are associated with a flat back which sometimes presents a dysplastic aspect as in this patient. Respiratory repercussions are frequent. |
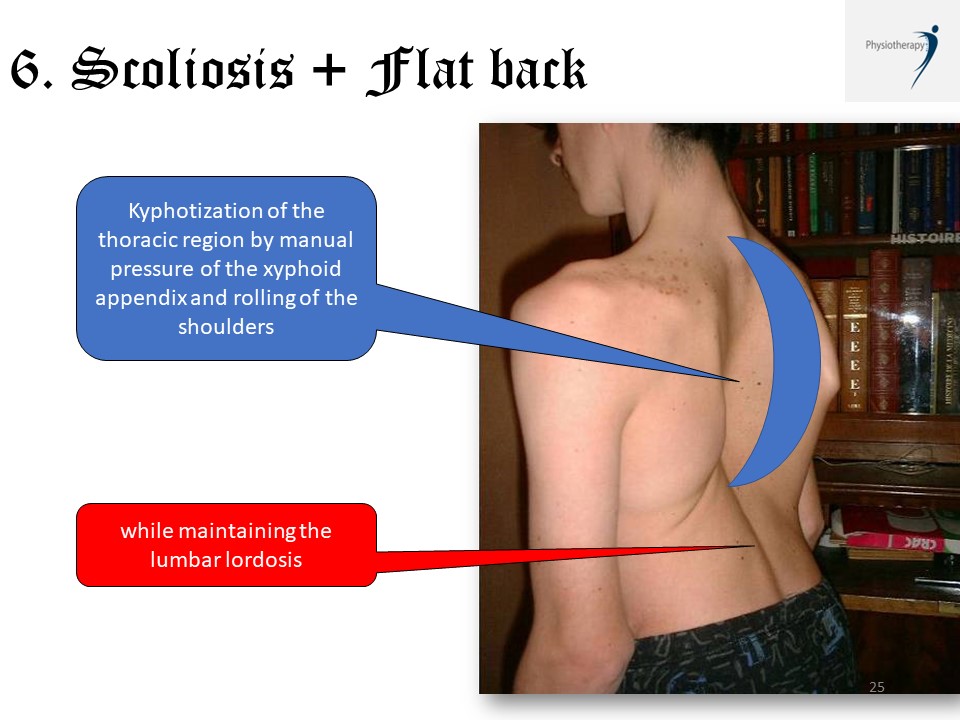 |
Kyphotization is difficult, especially since it is important to maintain lumbar lordosis.
|
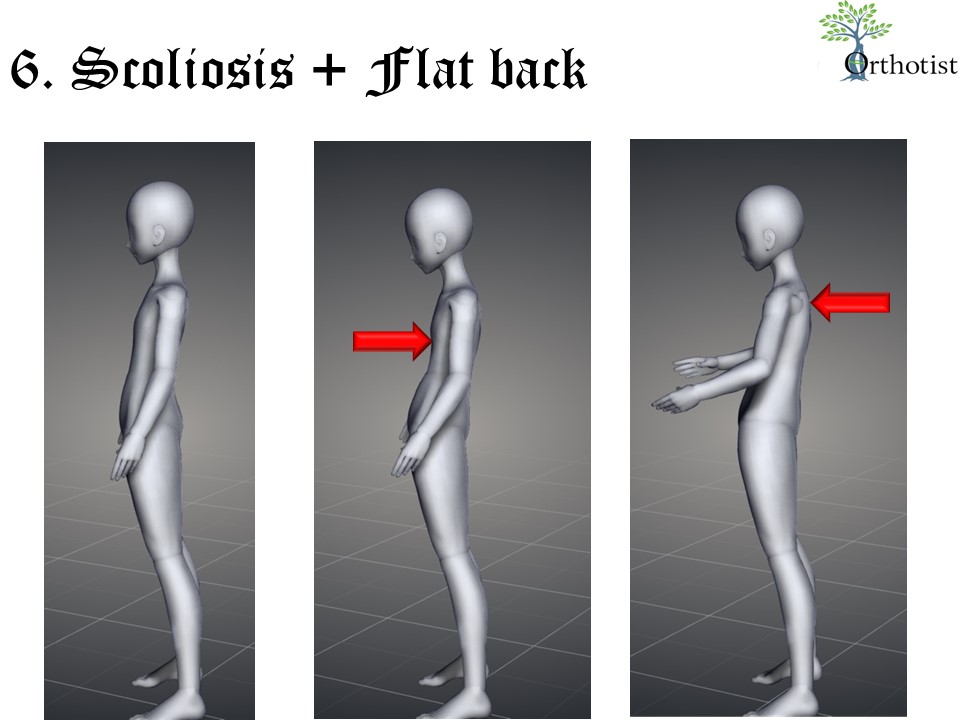 |
However, the ARTbrace allows an average improvement of about ten degrees during the treatment. The scan 3 is performed by maintaining pressure on the xyphoid appendage and asking the patient to roll up the shoulders. |
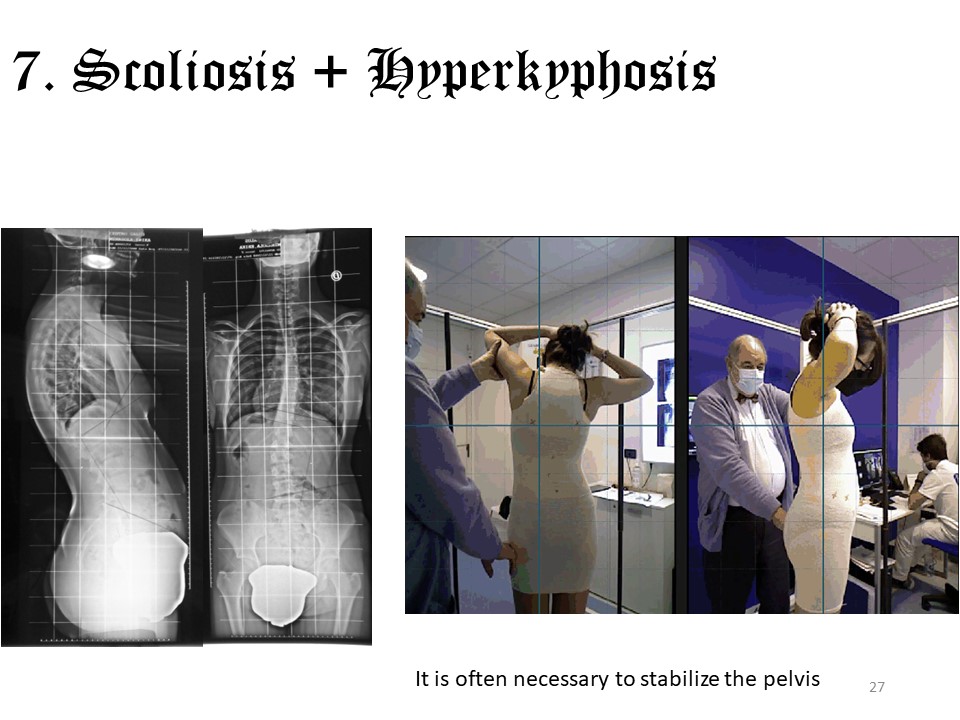 |
Scoliosis can also be associated with hyperkyphosis, especially in adults. In adolescents, it is often an asymmetric Scheuermann's disease associated with stiffness. Physiotherapy will therefore insist on the softening of the curves. The ARTbrace remains the indication of choice to manage both curves. We have found that scoliosis continues to progress in a brace that corrects the kyphosis alone. |
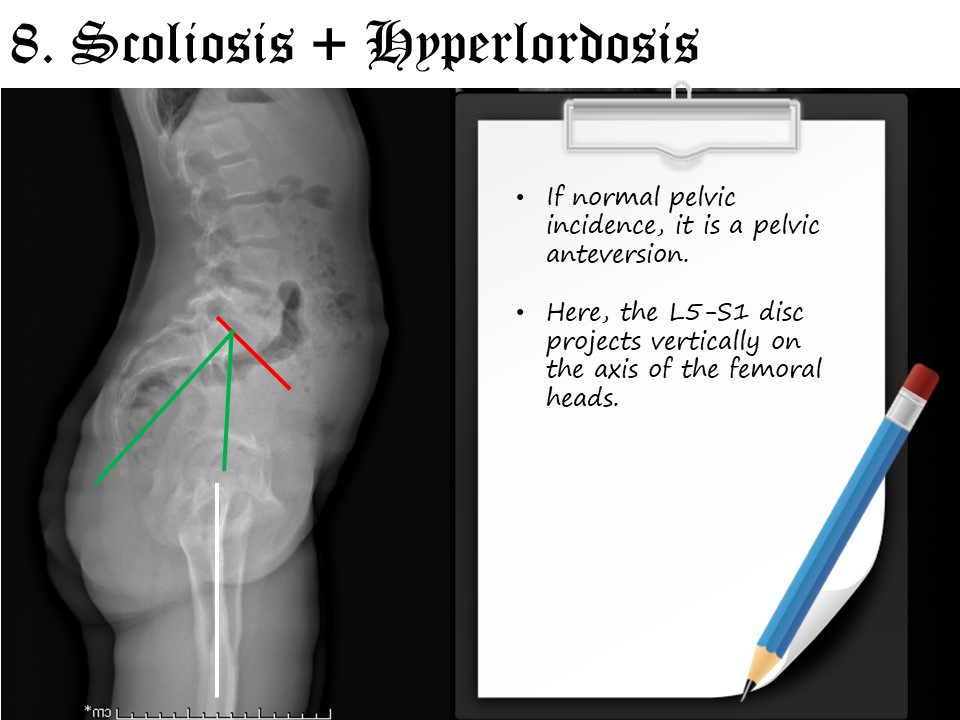 |
Scoliosis can also be associated with hyperlordosis. If the pelvic incidence is normal, it is a hyperlordosis by pelvic anteversion and the L5-S1 disc projects on the axis of the femoral heads. |
 |
The anteversion muscles such as the quadratus lumborum, iliopsoas and rectus femoris are stretched. Myotensive techniques may be indicated to the patient for daily home exercises. On the contrary, retroversing muscles such as abdominal, glutes and hamstrings will be strengthened.
|
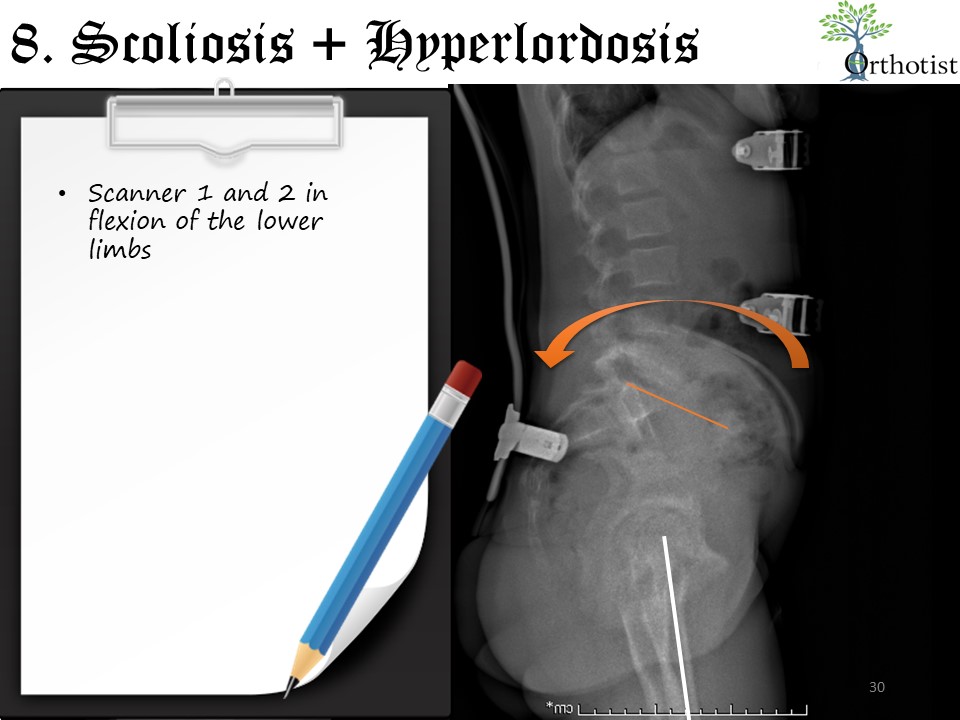 |
During scan 1, it is sometimes impossible to obtain correction of anteversion because of retractions. In this case, scan 2 will be performed with flexion of the lower limbs and during the superposition, hyperlordosis and anteversion will be corrected simultaneously. When the pelvic incidence is high, the lordosis automatically increases. A brace should only be used if the lordosis angle is greater than the pelvic incidence would like. |
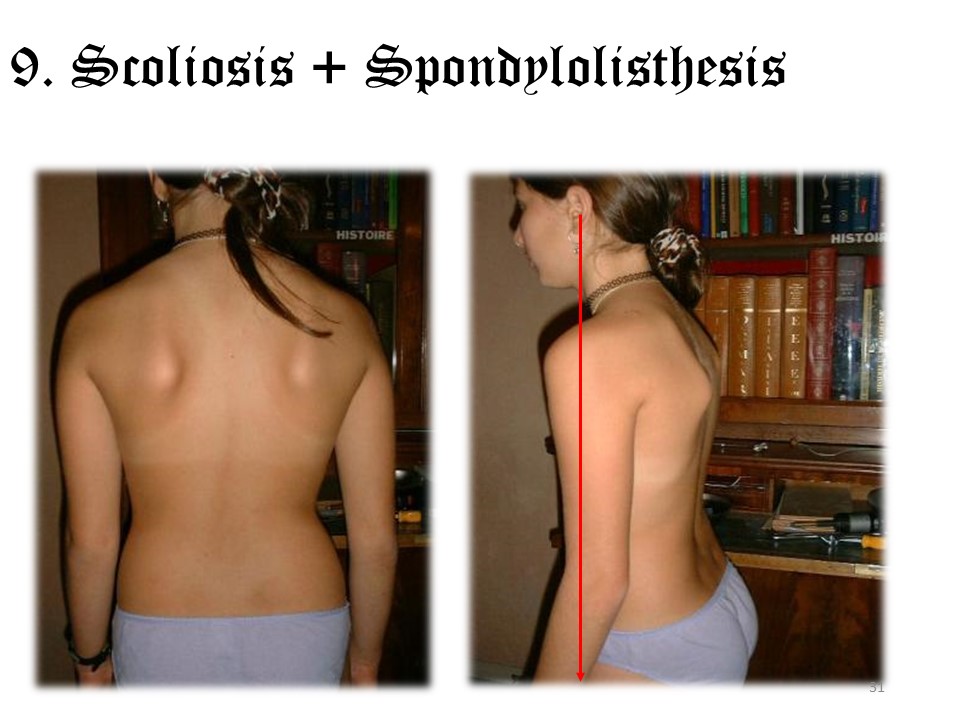 |
When there is spondylolysis or spondylolisthesis, which is the case for about 20% of lumbar scoliosis, the posture is often that of a symptomatic scoliosis with forward projection of the trunk. |
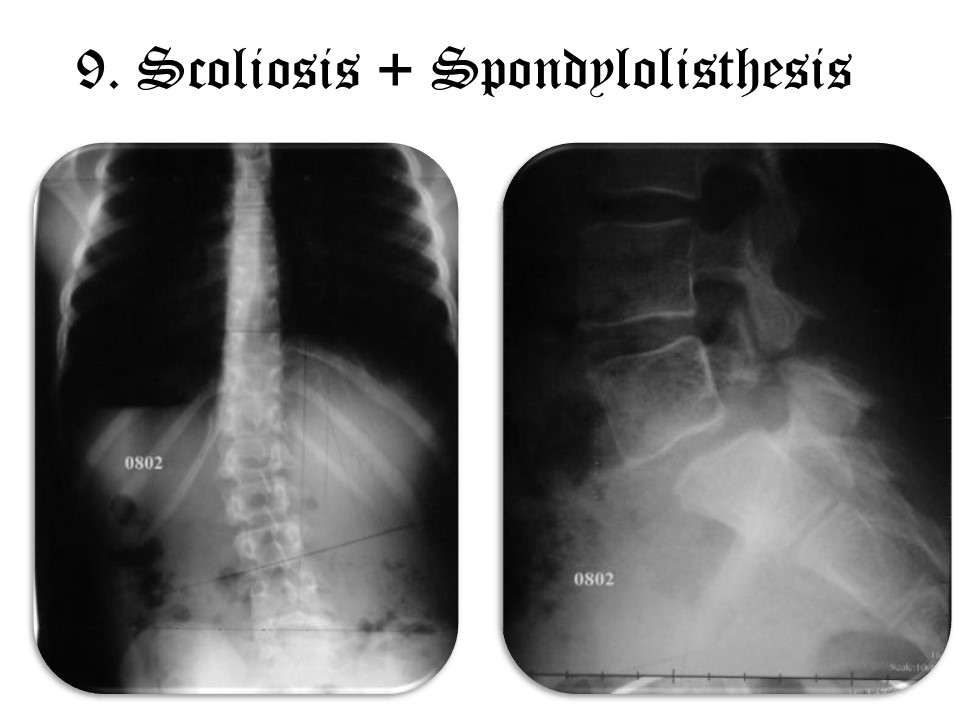 |
The rupture of the isthmus is not simultaneous and the frontal deviation occurs on the side of the first rupture. |
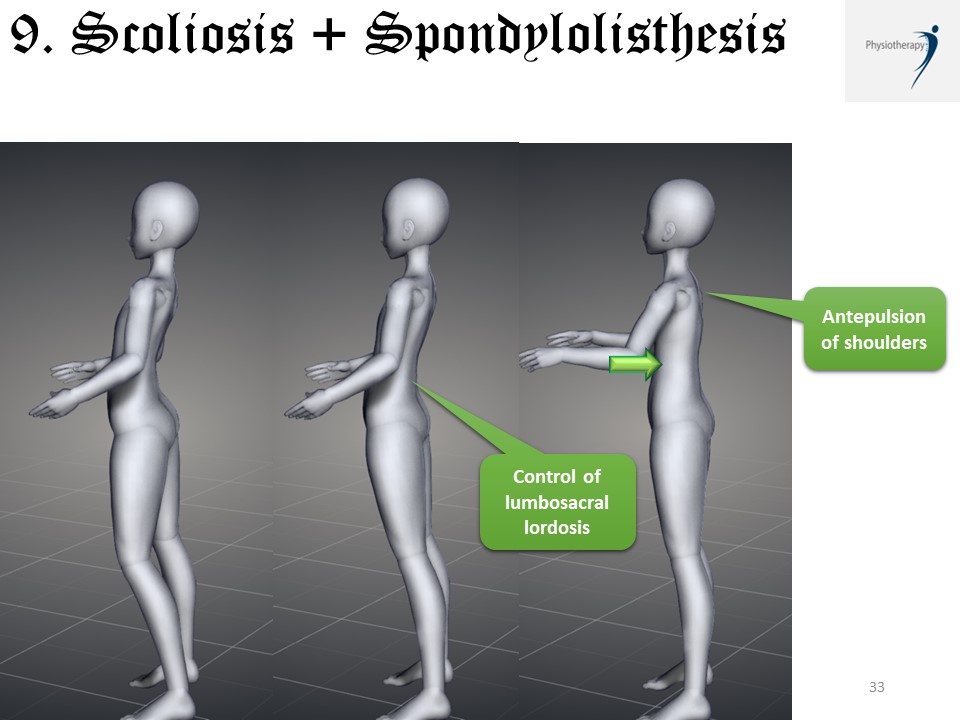 |
Olisthesis is often accompanied by a hyperlordosis that must be corrected while maintaining the lumbosacral lordosis to avoid verticalization of the sacrum. The correction is therefore performed on the upper part of the lumbar spine and associates extension of the spine by asking the patient to pull in the belly and to roll the shoulders forward.
|
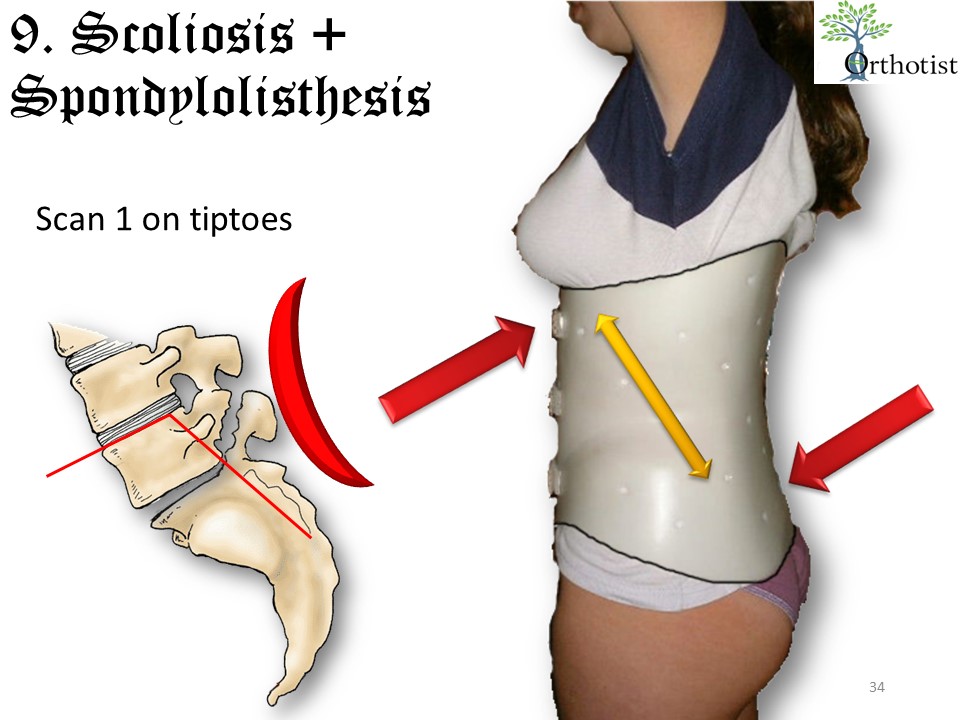 |
The corrective position is identical in a brace. Lumbosacral lordosis can be facilitated by having the patient stand on tiptoe during the scan. |
 |
The imbalance of the occipital axis can occur in the 3 planes of space. It is very frequent in adults. During the growth period, it reflects a significant asymmetry that exceeds the possibilities of correction of the postural system. |
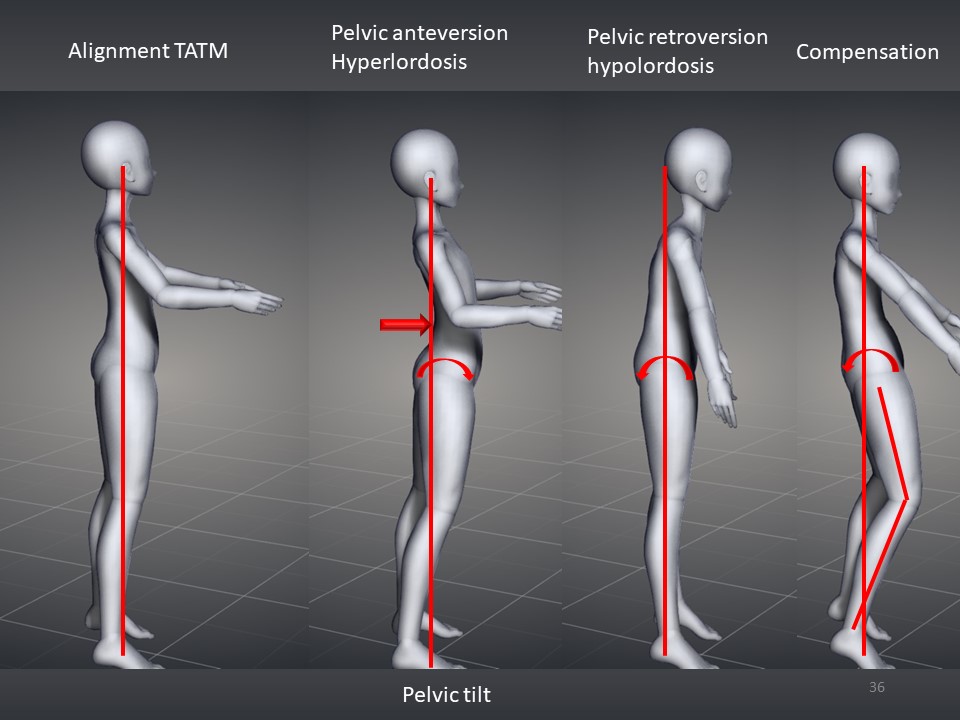 |
In a normal situation, there is an alignment between the tragus, acromion, trochanter and malleoli. The pelvic version must be determined in relation to the incidence. In adults, the most frequent situation is pelvic retroversion, which will be compensated by knee flexion to restore alignment. |
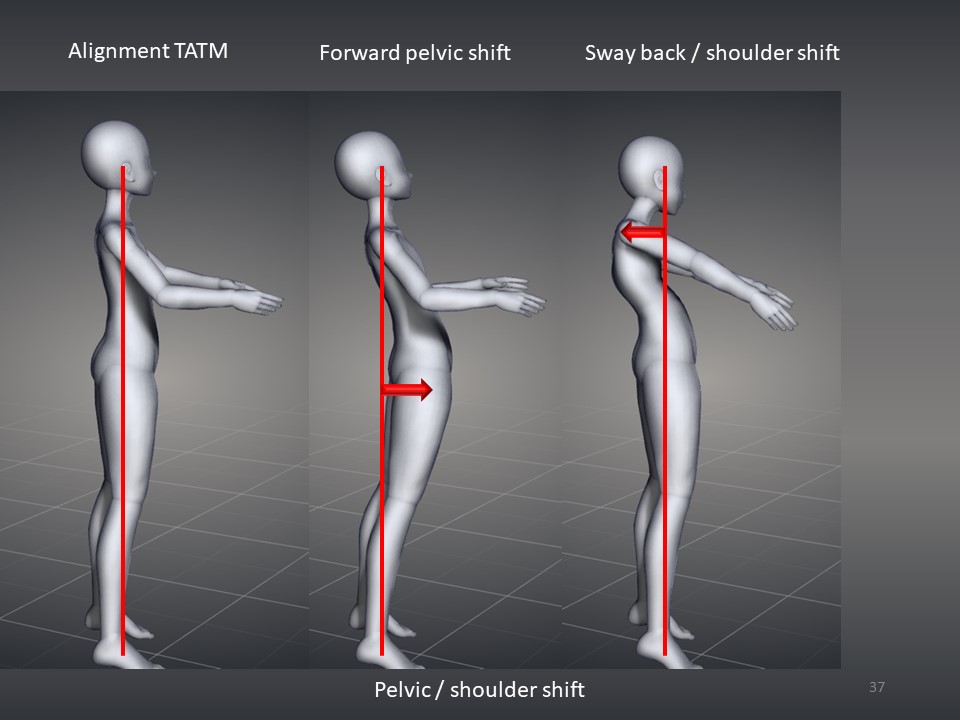 |
If the pelvic version is normal, it is often a translation along the sagittal axis at the pelvis or shoulders. For instance forward pelvic shift or backward shoulder shift like sway back.
|
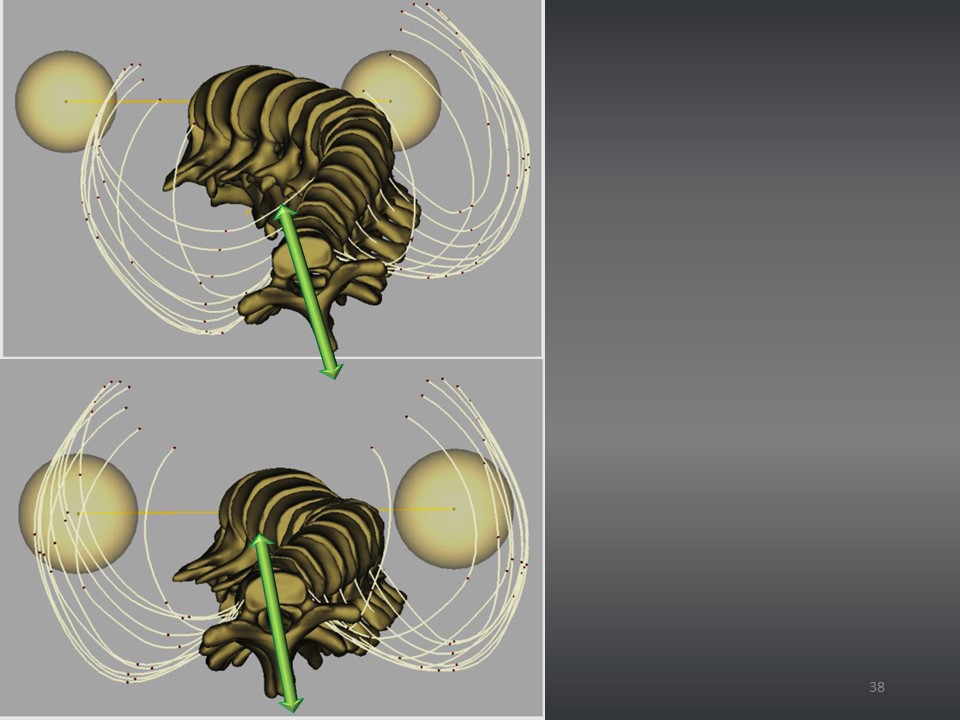 |
In the horizontal plane, the rotation of the pelvis is measured by the projection of the iliac wing on the frontal radiograph. Clinically, the rotation of the shoulder girdle in relation to the pelvic girdle is assessed. The EOS 3D system allows for accurate measurement of T1 rotation. |
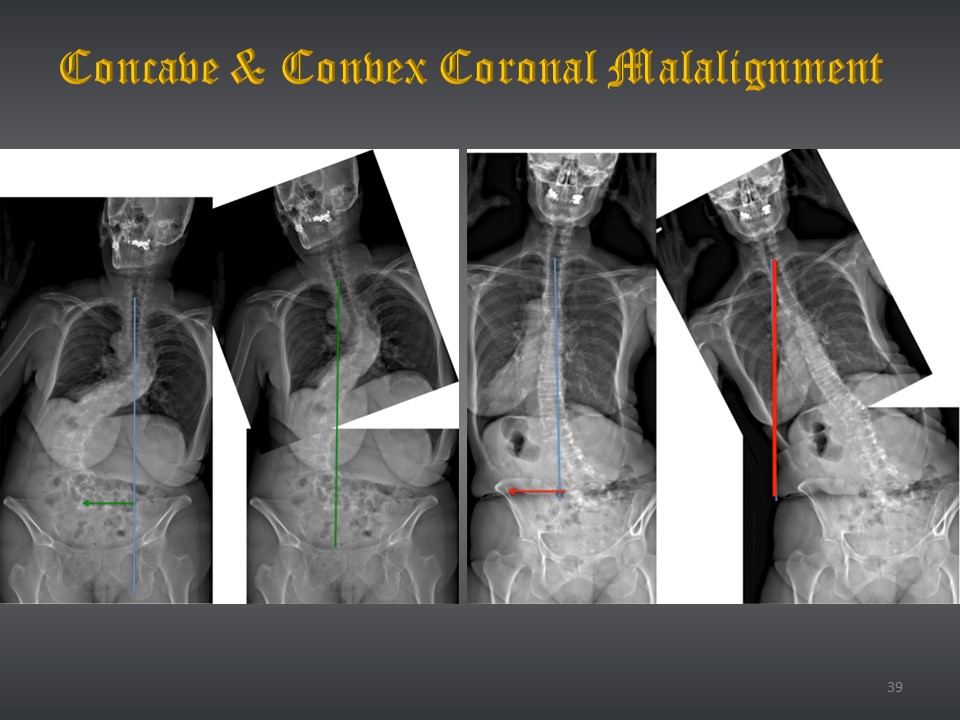 |
In the frontal plane, the imbalance is determined in relation to the concavity or convexity. We see on this montage realized by the authors of the article the good realignment in case of concave malalignment, and on the contrary the accentuation of the imbalance in case of convex malalignment, when one tries to correct the scoliosis. |
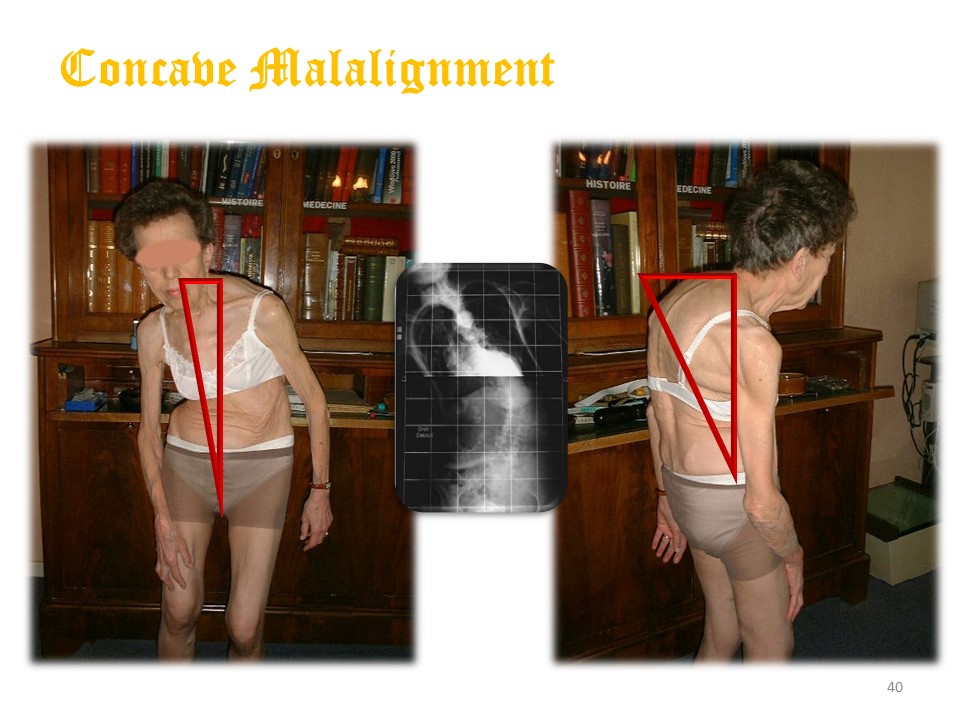 |
This is a typical case of concave malalignment. The patient is balanced only at the cost of stabilization with support on the right thigh. In addition to scoliosis, this patient presents with a high thoracic kyphosis of the osteoporotic type. |
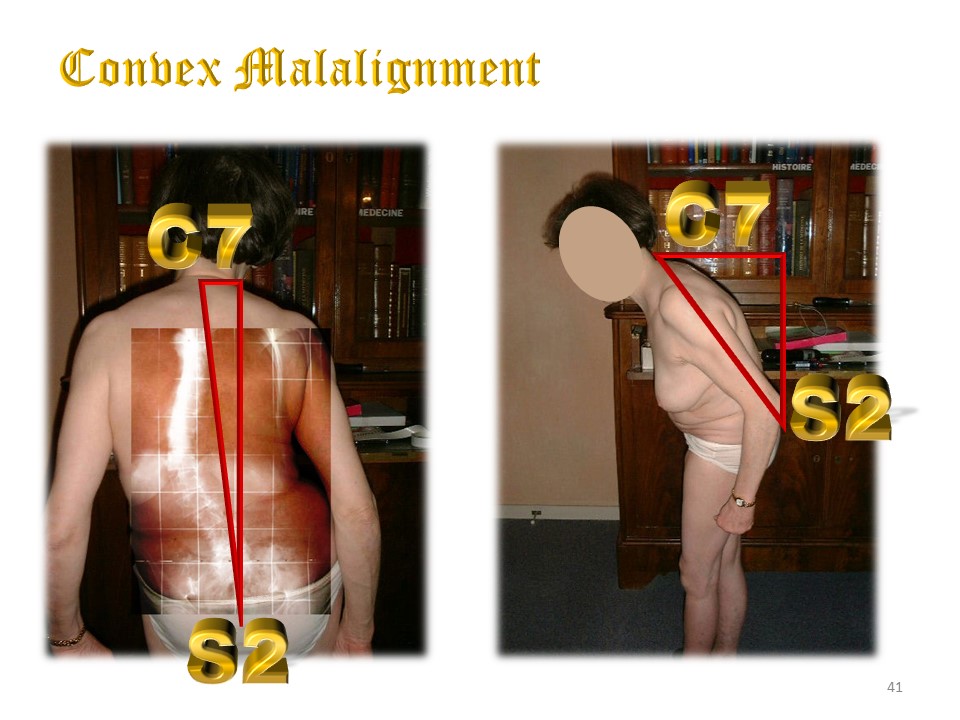 |
This is a typical case of convex malalignment. The correction of scoliosis is illusory. It is necessary to translate the lumbar spine on the line of gravity by a shift and the use of an adult ARTbrace with an iliac plateau. It will also be necessary to rebalance the sagittal plane by lordosing the lumbar region as much as possible.
|
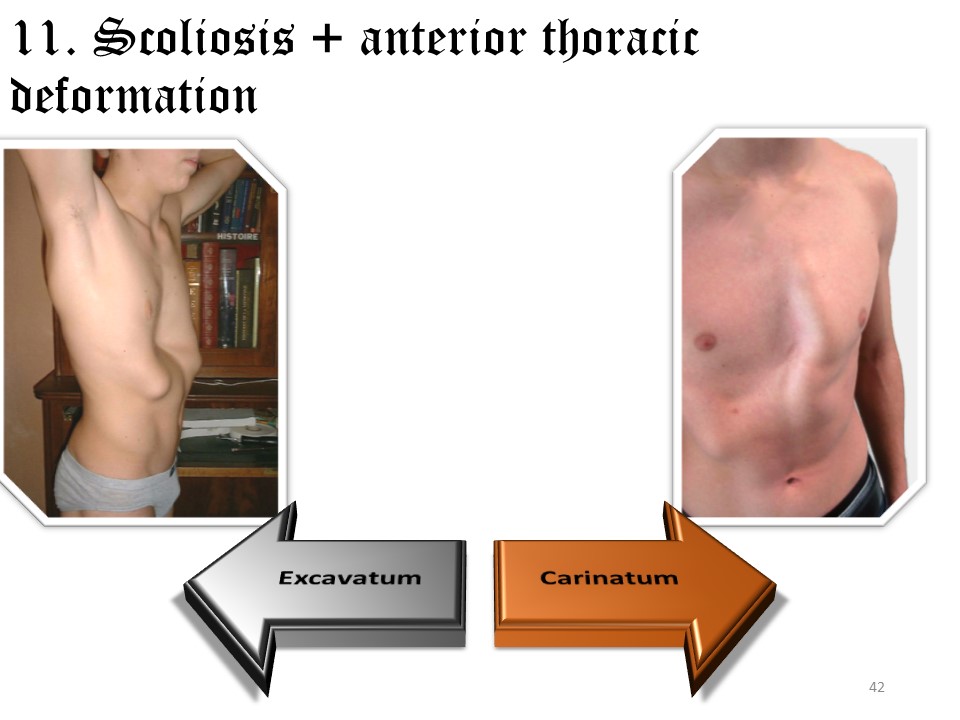 |
Anterior thoracic deformities are frequently associated with dysplastic scoliosis. A distinction is made between pectus excavatum and pectus carinatus, which are often asymmetrical. Pectus excavatum can lead to cardiopulmonary lesions that justify surgical treatment. For weaker deformities, there is a protrusion of the chondro-costal awnings that can be shaped by a brace. In girls, the development of the breast will mask the deformity. In boys, the brace will improve the aesthetic aspect. The consequences are more aesthetic and psychological than functional. |
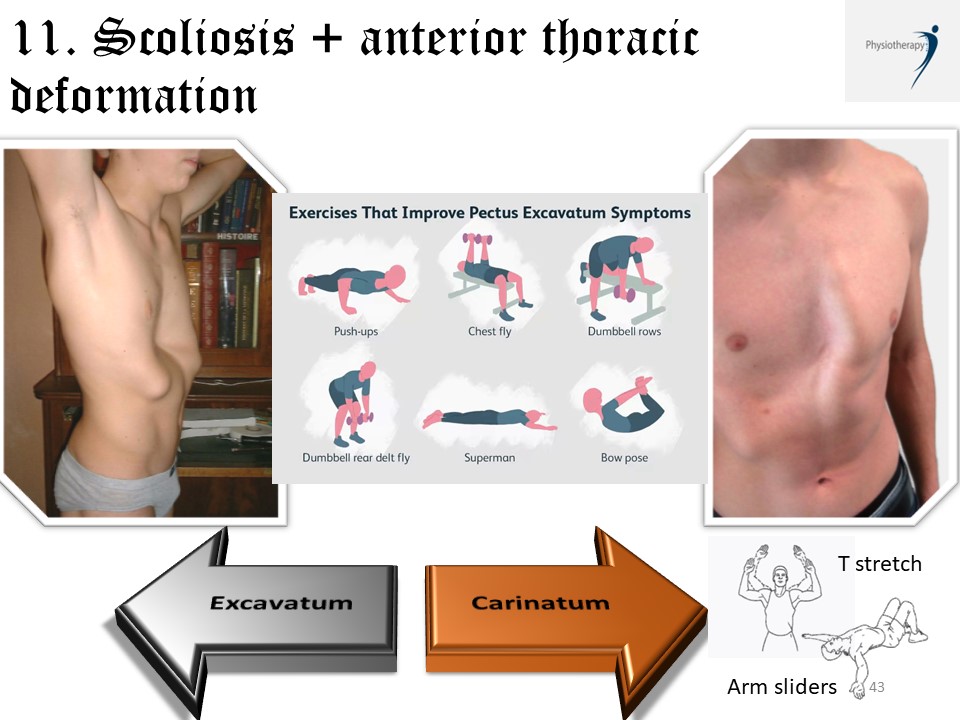 |
The objective is to stretch the rib cage and strengthen the transversus abdominalis muscle. For pectus excavatum: Push-ups, chest fly, dumbbell Row, Dumbbell rear delt fly, superman, & bow pose, can be done. For pectus carinatum: Arm sliders in standing, and T stretch on floor Forced inspiratory apnea/ stretching Musculation of the transverse abdomen Webbing of chondro-costal awnings The suction bell must be used 2 times 30' a day to be effective, which is very restrictive. swimming |
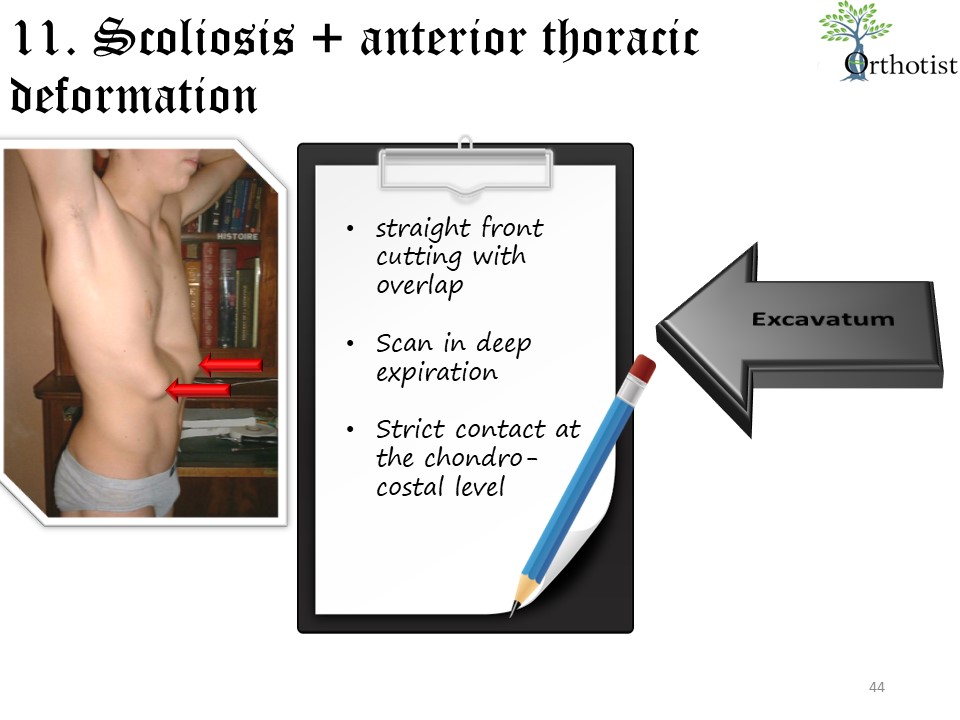 |
Treatment with a brace can be combined with treatment of scoliosis. Contact is made at the chondro-costal awnings and the carina. The anterior overlap with a straight vertical cut in boys allows for precise adjustment. Initial permanent wear is 6 weeks. Partial wear is determined by the angulation of the scoliosis. |
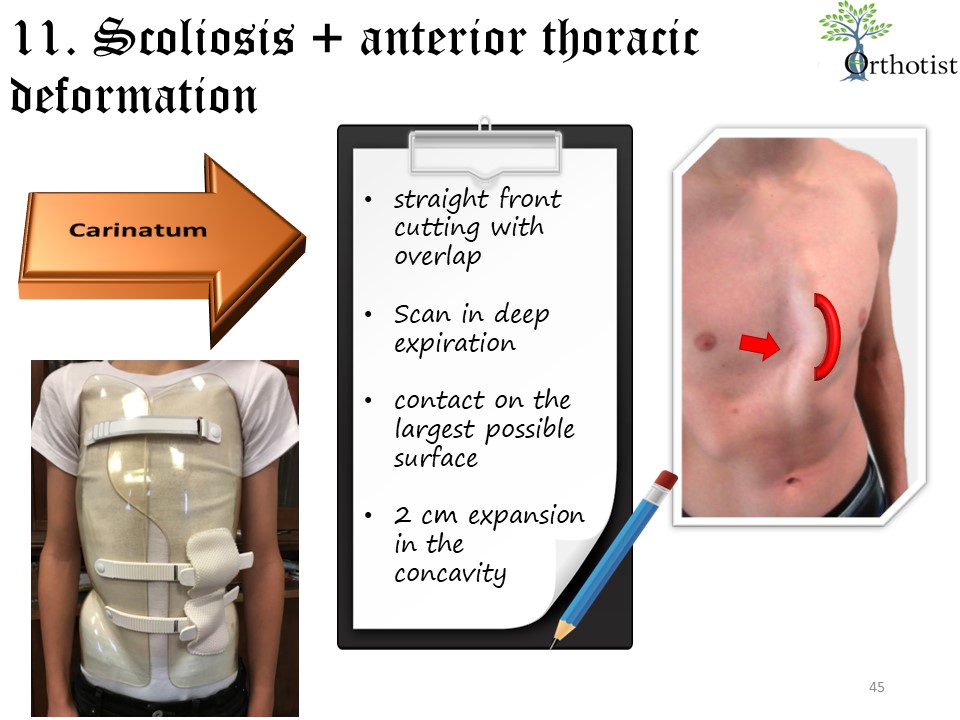 |
Symmetrization of the thorax is achieved by a concave expansion of at least 2 cm. Scans 1 and 3 are performed during deep expiration in order to model during inspiration. After 6 months, a pad will perform a progressive shaping.
|
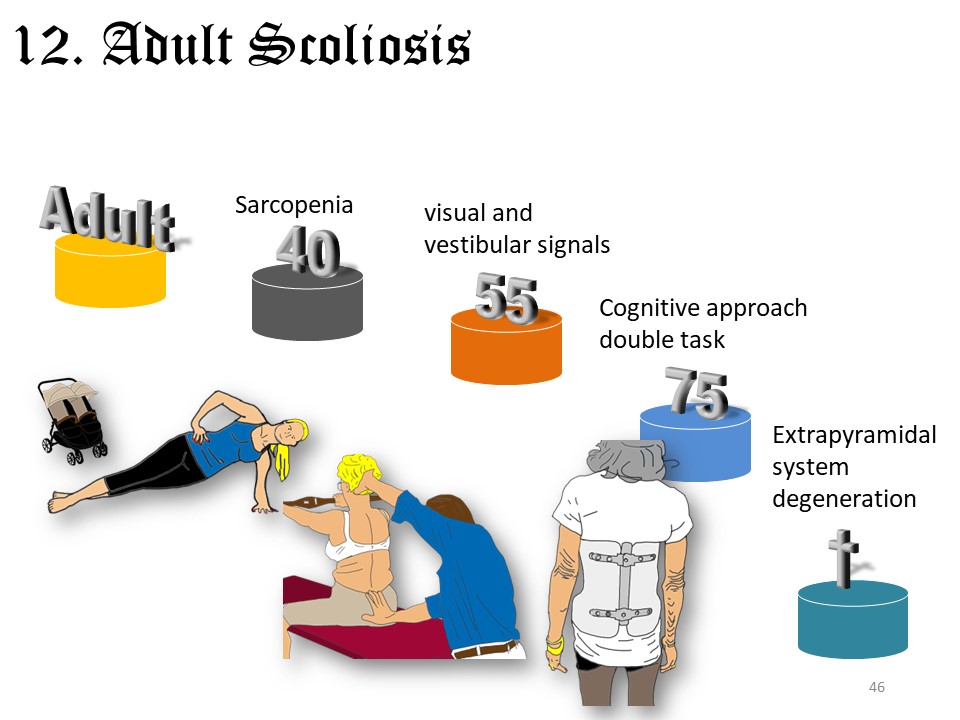 |
Adult scoliosis is currently a rapidly developing chapter. The Lyon method follows the evolution of the postural system with a first muscular stage at 40 years of age, the disturbance of visual and vestibular signals after 55 years of age, the cognitive disorders after 75 years of age and finally the atrophy of the axial musculature with the Pisa syndrome and the camptocormia. |
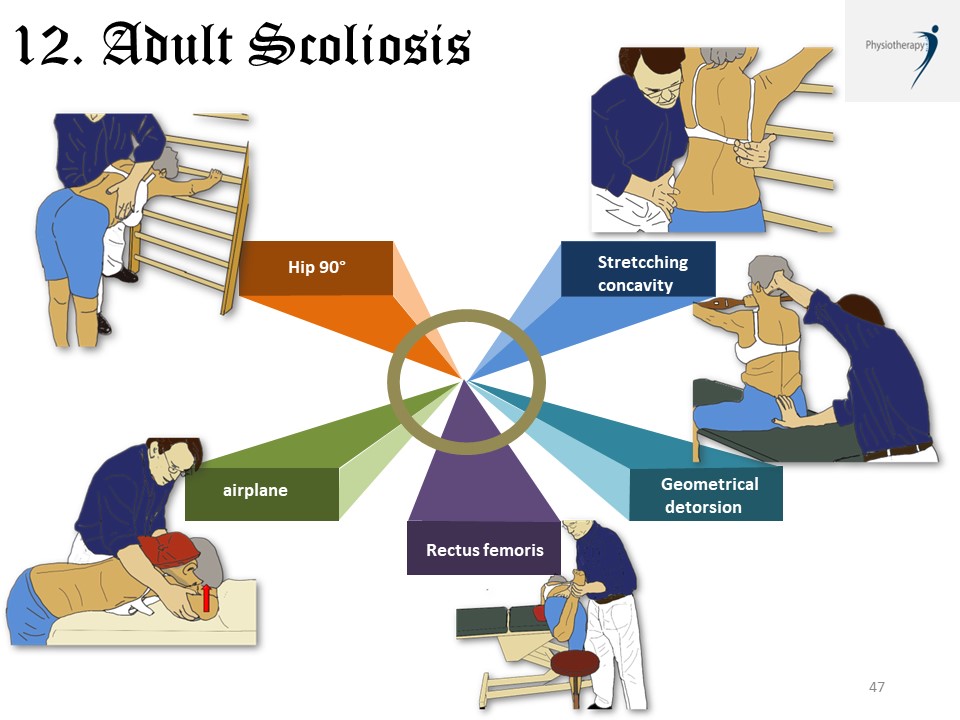 |
The main characteristics of adult scoliosis are: 1. Position with hips flexed to 90° in a closed kinetic chain for better relaxation of the pelvi trochanteric muscles and better control of lordosis. 2. Active and activo-passive concave stretching at the apex of the scoliotic curvature, 3. Geometrical detorsion in isostatic balance with visual feedback using the level stick in the absence of thoracic hyperkyphosis. 4. Stretching and strengthening of the rectus femoris to promote pelvic anteversion 5. Strengthening of the extensors at the cervico-thoracic level by the exercise of the plane in retropulsion of the shoulders. |
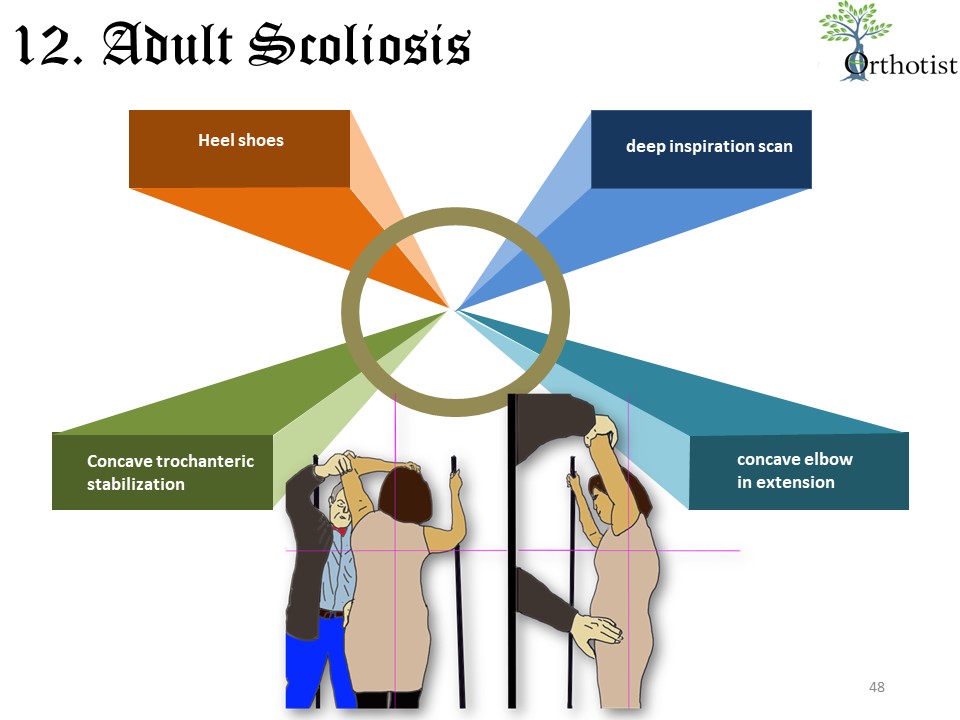 |
The realization of the brace is also different. It is most often made in one step. Heeled shoes favor the lumbar lordosis during the casting. The patient is asked to take a deep breath and to shrug his shoulders while placing the concave hand on his head. In the sagittal plane, the concave elbow is in maximum antepulsion to correct the thoracic kyphosis and often a trochanteric stabilization is useful for a perfect frontal alignment. The position is identical to that of CT 2 of an adolescent thoracolumbar curve. The criteria of reducibility are essential to improve the acceptability of the brace. |
 |
The multiplicity of particular cases makes complex classifications illusory and undoubtedly explains the variability of results both in terms of physiotherapy and braces. A simple mechanical correction in the sagittal plane and then in the frontal plane associated with a postural stimulation adapted to the patient's age makes it possible to take into account all the particular situations.
|
The pelvis is an intermediate vertebra between the spine and the lower limbs. In the frontal plane 5 concepts must be considered: 1. Lumbosacral Scoliosis with Asymmetric Structural Anomaly of the Lumbo-Iliac Junction (ASALIJ) which will be treated by opening the ilio-lumbar angle. 2. Lumbopelvic scoliosis with included or excluded pelvis. The existence of an included pelvis requires an underarm brace, while the excluded pelvis allows the use of a short brace. 3. Exposed hinge with the bicrested line intersecting L5 which promotes disc degeneration and prevention. 4. Uneven pelvis (LLD) and functional scoliosis with the problem of compensation by shoe lift. 5. Coronal imbalance either convex or concave. The restoration of convex imbalance is done by geometric detorsion, concave imbalance by mechanical detorsion. Numerous clinical cases will illustrate these concepts, as each patient may have several anomalies that will guide the physiotherapy and the choice of brace.