Exercise: Past, Present & Future (Part 1)
Inappropriate treatment of adolescent idiopathic scoliosis can result in serious health problems. Growing evidence indicates that specific exercises may be more effective in managing adolescent idiopathic scoliosis.
Vaiva Selevicien, Lithuania
 |
The journey of scoliosis-specific exercises from the past to the present, and extending into the future, remains a singular narrative. Although the transition from empirical understanding to data-driven evidence has occurred, the core objective and foundational principles have remained steadfast. While the methods may differ and evolve based on regional capabilities and the characteristics of scoliosis itself, a historical overview reveals an invisible continuum—an enduring thread that connects generations across the last two hundred years. In the earlier era, scoliosis caused by rickets and infections was prevalent, marked by severe curvatures that are rarely seen today. In our current time, we identify patients with milder curvatures, and looking ahead, we aspire to tailor exercises precisely to address the root causes of scoliosis. |
 |
Throughout history, numerous researchers have made significant contributions to the field of physiotherapy, leaving an indelible mark on its development. Among the most renowned figures are Charles Gabriel Pravaz, Rudolf Klapp, Katerina Schroth, Min Mehta, Marianna Bialek, and Michele Romano. Each of these distinguished individuals has enriched the discipline with their unique exercises and specialized knowledge, advancing the practice in remarkable ways.
|
 |
The pioneering institution dedicated to the treatment of spinal deformities was located in Switzerland and founded by Venel. Meanwhile, in France, the most renowned center is in Lyon, established by an orthopedic doctor but also engineer credited with inventing the syringe. Besides the main structure, the swimming pool can be observed at the bottom left.
|
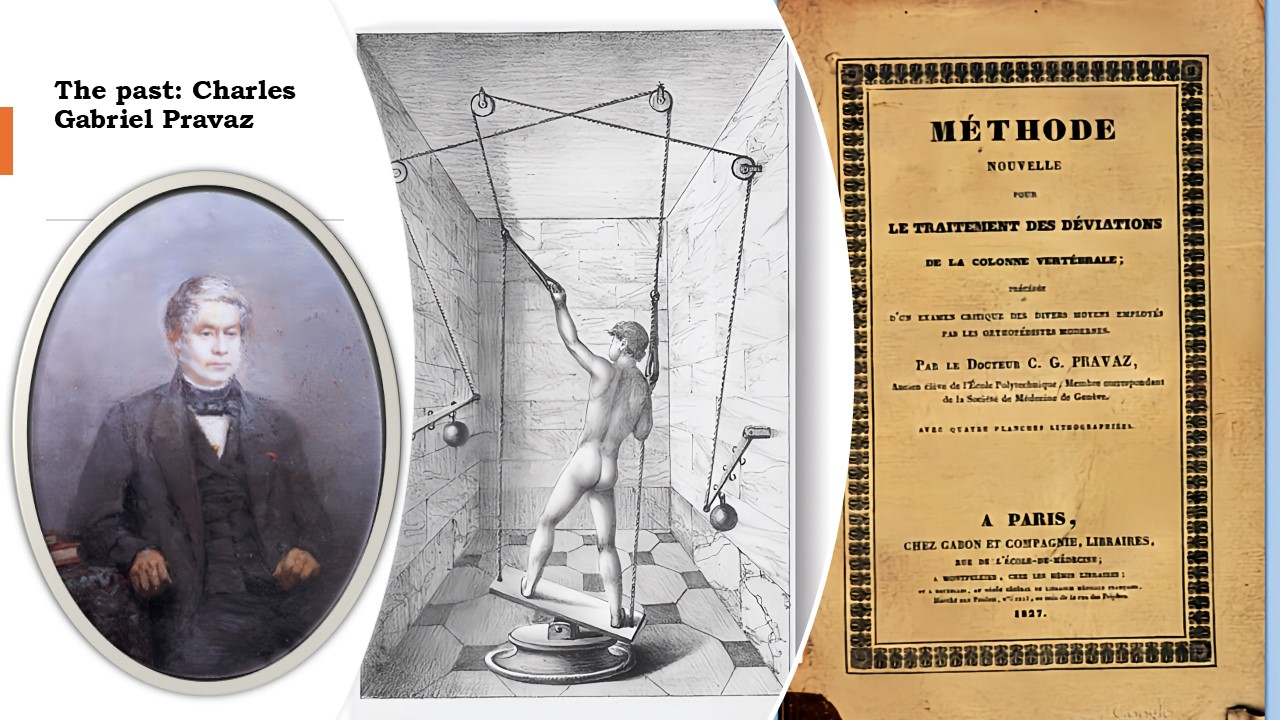 |
The origins of specific exercises designed to counteract scoliosis can be traced back to the early 1800s. These exercises were meticulously detailed and depicted in the pioneering work on scoliosis physiotherapy by Charles Gabriel Pravaz, the visionary behind the Lyon Method, which offers a non-invasive approach to treating scoliosis. His book, adorned with intricate engravings, presents a method where the spinal curve is realigned through the strategic use of stretches and resistance, utilizing weights and pulleys. Additionally, an innovative device—a tilting platform known as the orthopedic swing—was employed beneath the feet to activate the extrapyramidal system. This marked the inception of exercises focused on enhancing balance. |
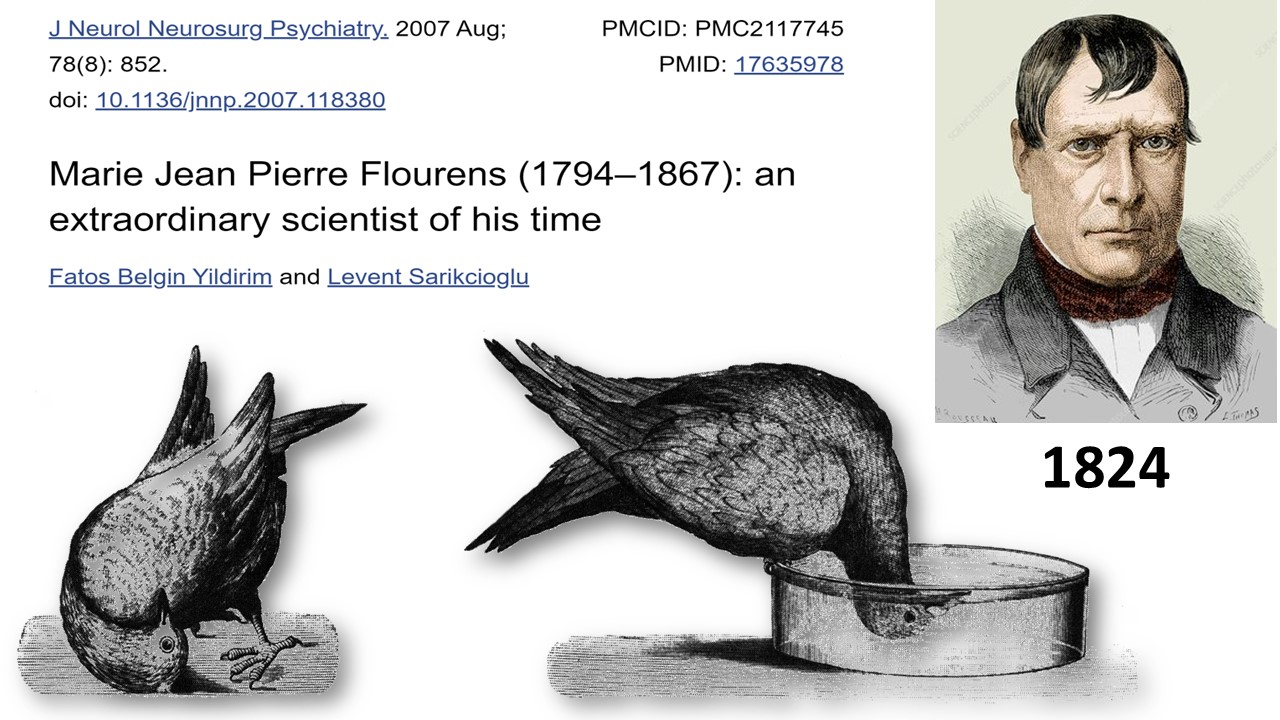 |
In the annals of history, the initial connection between scoliosis and the extrapyramidal system was established by a renowned French physiologist named Jean Pierre Flourens. It was in the year 1824 that Flourens unveiled his pioneering research on pigeons afflicted with scoliosis following the obliteration of the labyrinth. Contrary to his original anticipation of merely inducing deafness, this groundbreaking study paved the way for a deeper understanding of the physiological interplay. |
 |
Back in those days, braces were not yet available, so the approach to treatment included both nocturnal traction while in bed and the use of mechanical devices during the day. These devices aimed to rectify the curvature by expanding and straightening the concave areas, an aspect that remains integral to the Lyon Method even today. |
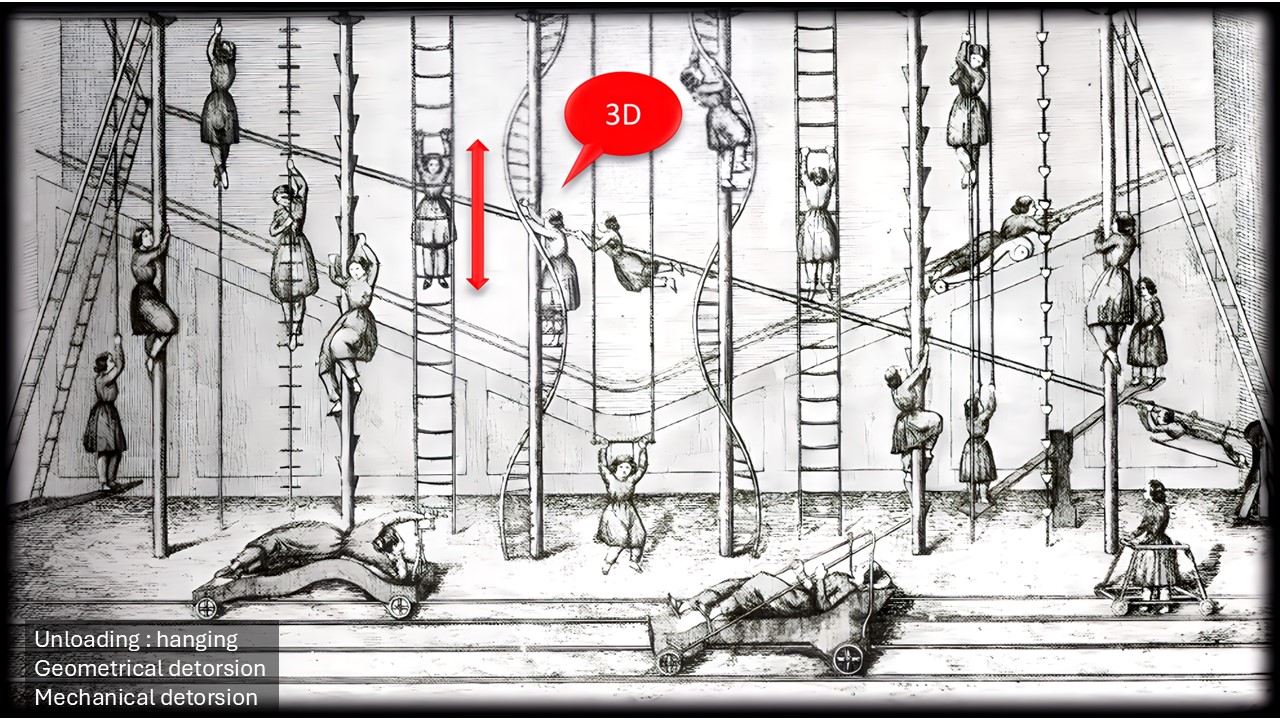 |
Mechanical adjustments are enhanced through exercises focused on self-stretching or geometric detorsion. The notion of three-dimensionality was widely recognized, with helicoidal staircases reinforcing the spiral structures. |
 |
Aquatic sports served as an excellent supplement to land-based workouts, aiding in the rectification of flat back issues within the sagittal plane. The synergy between mechanical adjustments—typically achieved through the use of braces—targeted exercises, and athletic activities continues to be the standard approach in most treatment methodologies. |
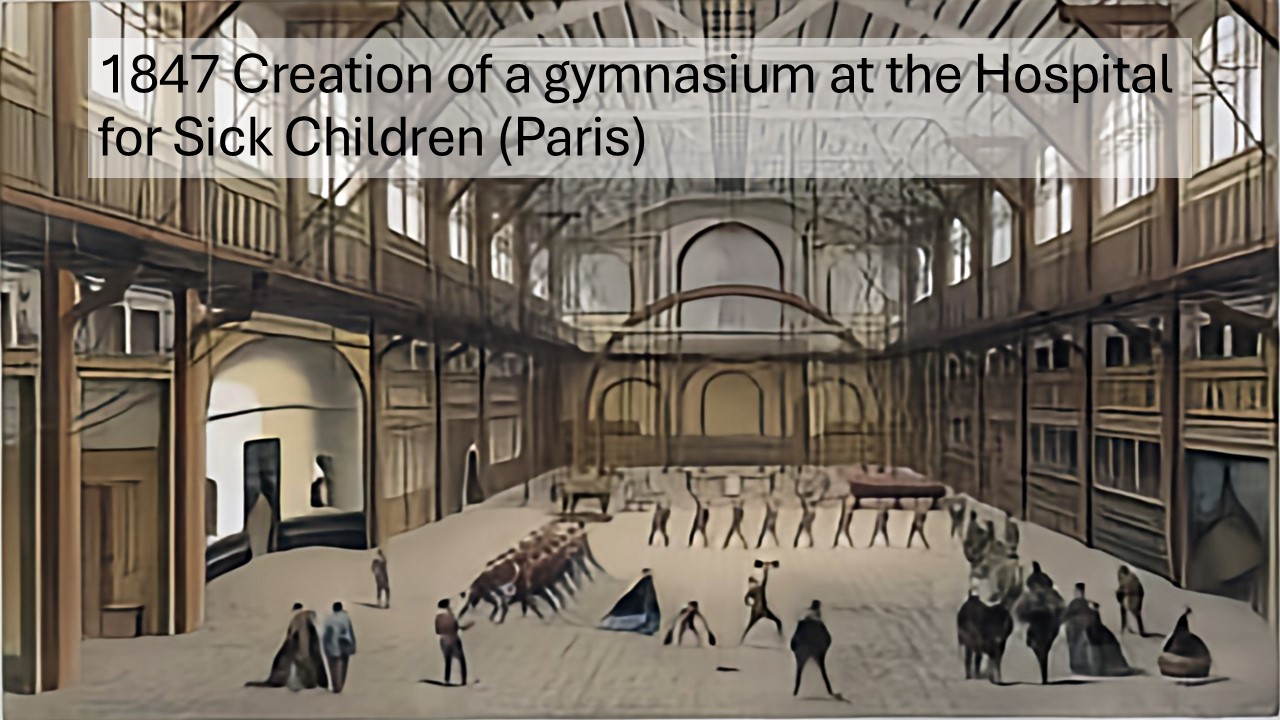 |
During the mid-1800s, the inclusion of gymnasiums within children's hospitals became increasingly common. In Lyon, the Faculty of Medicine founded by Rockefeller not only featured a gymnasium but also boasted a dedicated gymnastics instructor for the students. This gymnastic instructor would later become the first director of the physiotherapy school, which was seamlessly incorporated into the Faculty of Medicine. |
 |
A burgeoning fascination with medical gymnastics eventually gave rise to specialized institutions dedicated to orthopedics and massage therapies. At that time, the word 'physiotherapy' had not yet been introduced into the lexicon. |
 |
The pioneering outcomes of this form of exercises, which emphasize axial stretching and bending to open scoliotic concavity, were initially documented by Claude Bernard. Bernard, a renowned physician born in Lyon, is celebrated as the progenitor experimental medicine. |
 |
During that era, mechanotherapy was extensively employed in the fields of orthopedics and traumatology. A number of institutes initiated treatment for scoliosis using these methods. The machinery they relied upon was driven by steam boilers. It was from this very mechanotherapy that the modern disciplines of physiotherapy and the profession of physiotherapists emerged.
|
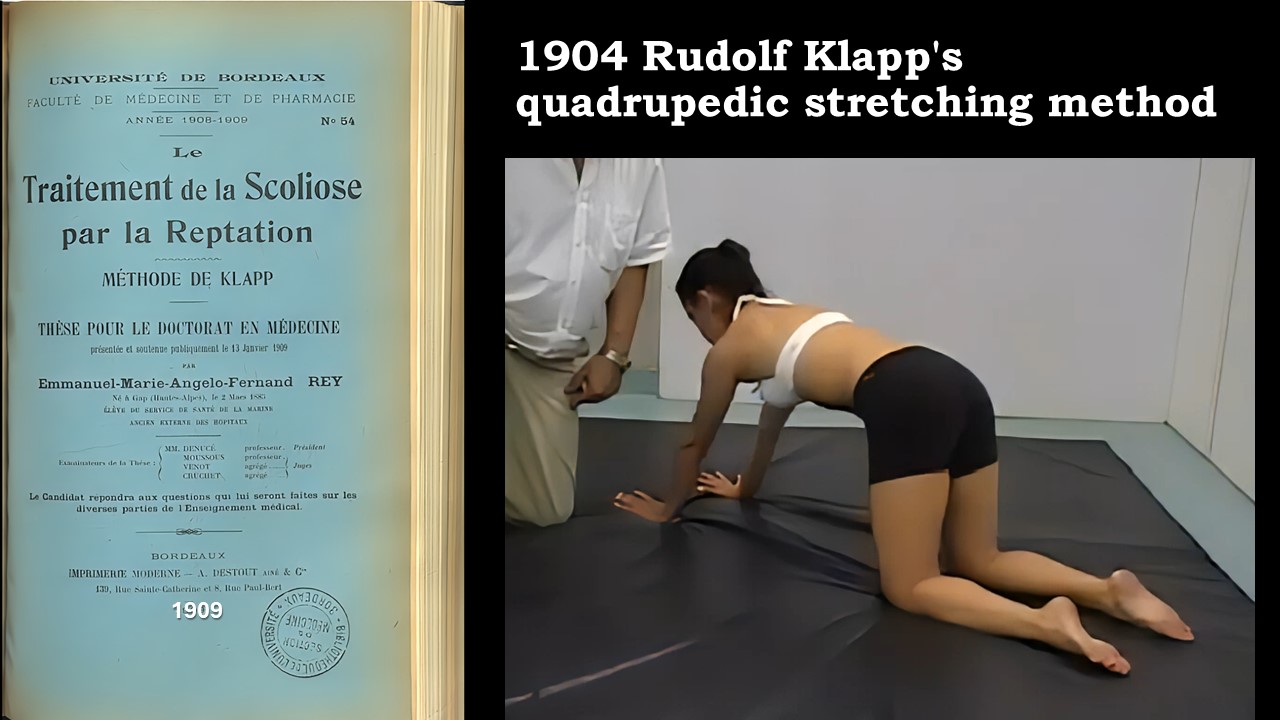 |
In Germany, dedicated facilities and therapists develop techniques centered on specialized exercises, including the quadrupedia mobilization method pioneered by Rudolf Klapp. This approach is grounded in the understanding that scoliosis is uniquely associated with bipedal locomotion. The lack of axial loading enhances the effectiveness of corrective bending. Mobilization is carried out sequentially across the three spatial planes.
|
 |
For a decade, Katherina Shroth dedicated herself to teaching gymnastics in Germany. Faced with the challenge of her own scoliosis, she innovatively developed a personal technique to replace the traditional brace that had been recommended to her. |
 |
Her first academic publications primarily explore the nuances of concavity-oriented breathing techniques during an era when polio-induced scoliosis was widespread. The condition frequently resulted in diaphragm weakness due to polio-induced muscle paralysis. |
 |
In the original Schroth program, mirror monitoring is pivotal in aligning corrective movements and postural awareness with visual feedback. This practice harnesses the power of the mirror to activate the tecto-spinal tract within the extrapyramidal system. The alignment of the head, trunk, and lower limbs is carried out in a non-vertical position, with a tilt directed toward the concave side. |
 |
The practice of geometric chin-strap detorsion is intricately linked with muscle cylinder exercises, which are performed while seated asymmetrically before a mirror, accompanied by controlled, derotatory breathing techniques, envisioned here in hues of blue. This method of self-extension employs the convexity of the upper limb to realign and level the uppermost vertebra. Utilizing a small bench for positioning enhances effectiveness. The muscular cylinder inclines towards the concavity, while the perpendicular alignment of the pelvis relative to the trunk's tilt facilitates the reorientation of the lumbar spine. |
 |
The stiffness at the apex of scoliotic curves exceeding 40° contrasts with the increased mobility found at the level of the limiting vertebrae. The concept involves tilting the apical vertebra towards the concavity and utilizing the hypermobility to restore the horizontal position of the limiting vertebrae at the shoulder and pelvis levels. A drawback is the compromise of the line of gravity during the exercise.. |
 |
In 1984, Min Mehta recommended that her patients adopt a snug, asymmetrical sitting position for several minutes each hour while at school. Taking the example of a right thoracolumbar curve, the corrective maneuver involves a combination of lateral lumbar translation or shifting, thoracic lateral bending, and axial extension, all while ensuring that the head remains aligned with the gravitational axis. |
 |
In 2004, Marianna Bialek introduced an exercise designed to fortify the spiral chain that extends from one shoulder across to the opposite hip, utilizing elastic bands for resistance. Nevertheless, engaging in this activity may inadvertently amplify stiffness, and it is noteworthy that in cases of idiopathic scoliosis, there is no deficiency in the pyramidal muscle. |
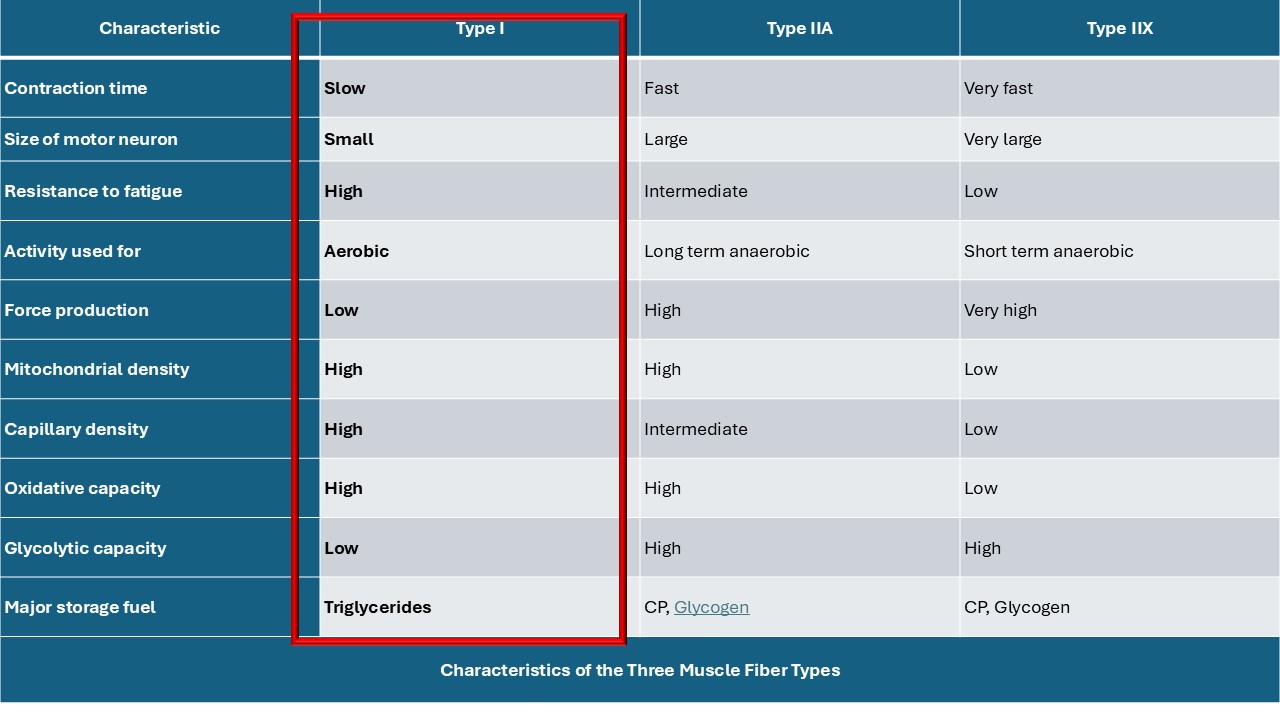 |
The deep axial musculature essentially comprises type 1 extrapyramidal muscle fibers. The superficial spiral chain with type 2 muscle fibers is not altered in scoliosis.
|
 |
Rotation movements cause significant issues at the intervertebral disc level, increasing flexion-rotation stresses by 400%. The most frequent complication in adulthood is rotatory disc displacement. Rotational ranges are very limited at the lumbar level. Consequently, the Lyon Method rarely employs direct rotations. Instead, it utilizes coupled movements to achieve rotation.
|
 |
Quite at the same time, Michele Romano introduced a refined version of the Lyon Method by incorporating a cognitive-behavioral perspective. This approach emphasizes achieving enhanced symmetry and integrating it as an intrinsic postural reflex. While the Lyon Method traditionally targets stimulation of the extrapyramidal system, SEAS aims to intricately develop a novel postural reflex. This is particularly significant, given that scoliosis appears to be associated with delayed maturation of the postural system, a topic we will explore further in the latter segment of this presentation. |
 |
It is highly advised against using neuro-enhancement techniques for youngsters and teenagers. |
 |
The abbreviation PSSE, which stands for Physiotherapy Scoliosis Specific Exercises, was introduced by Josette Bettany-Saltikov. By integrating more than six well-established physiotherapy techniques, a cohesive and agreed-upon approach to exercises tailored for scoliosis has been developed. |
 |
The primary exercises can be categorized into groups focusing on balance, axial stretching, curve correction, respiratory improvement, strengthening of axial muscles, and cognitive integration. These exercises are universally recognized across different methodologies. Since 1963, the Swiss ball, an innovation by Italian Aquilino Casini, has been incorporated into all of these approaches. Similarly, the foundational awareness of spinal deformities is consistently emphasized. |
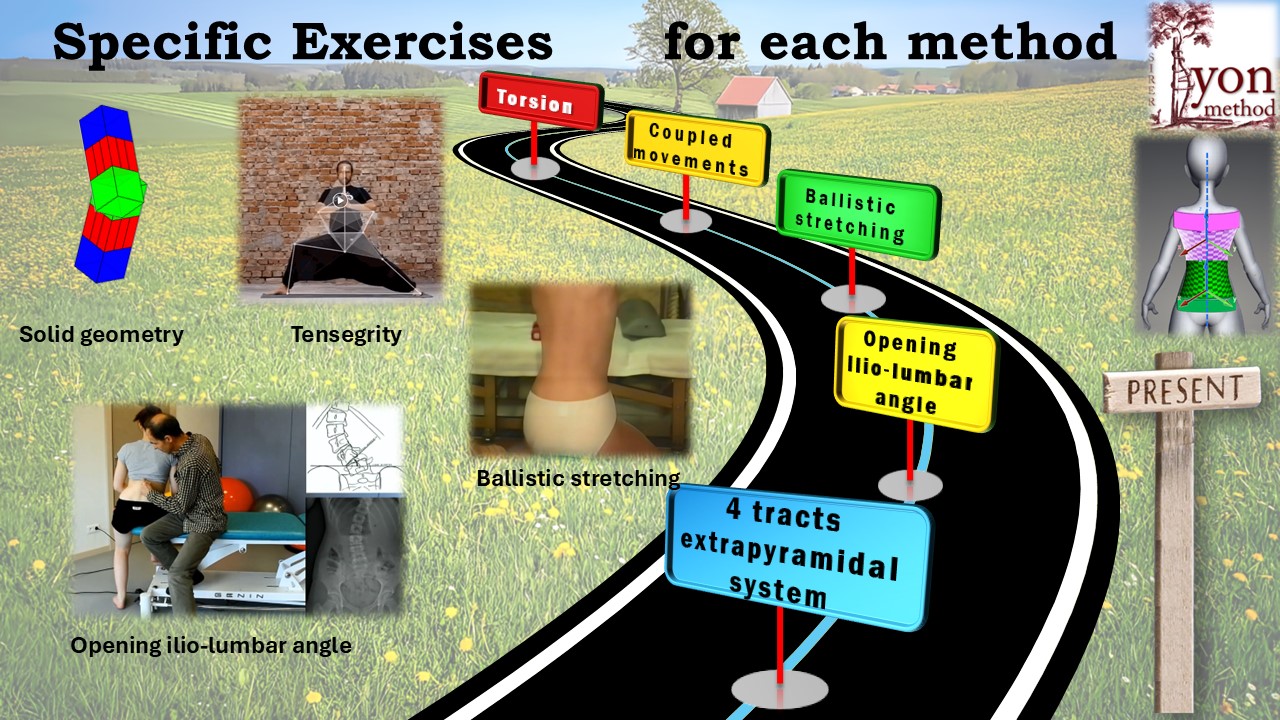 |
Each method is accompanied by exercises tailored to its unique approach. Take the Lyon Method, for instance; exercise number 5 focuses on expanding the ilio-lumbar angle, whereas exercise number 10 emphasizes ballistic stretching with the aid of a Swiss ball. Additionally, there are conceptual distinctions to consider, such as the reestablishment of Tensegrity when the body is in its corrected posture, and the idea of detorsion occurring between the stabilized scapular and pelvic girdles. Furthermore, the modeling techniques are distinct: the truncated parallelogram is supplanted by the hyperboloid of the trunck. |
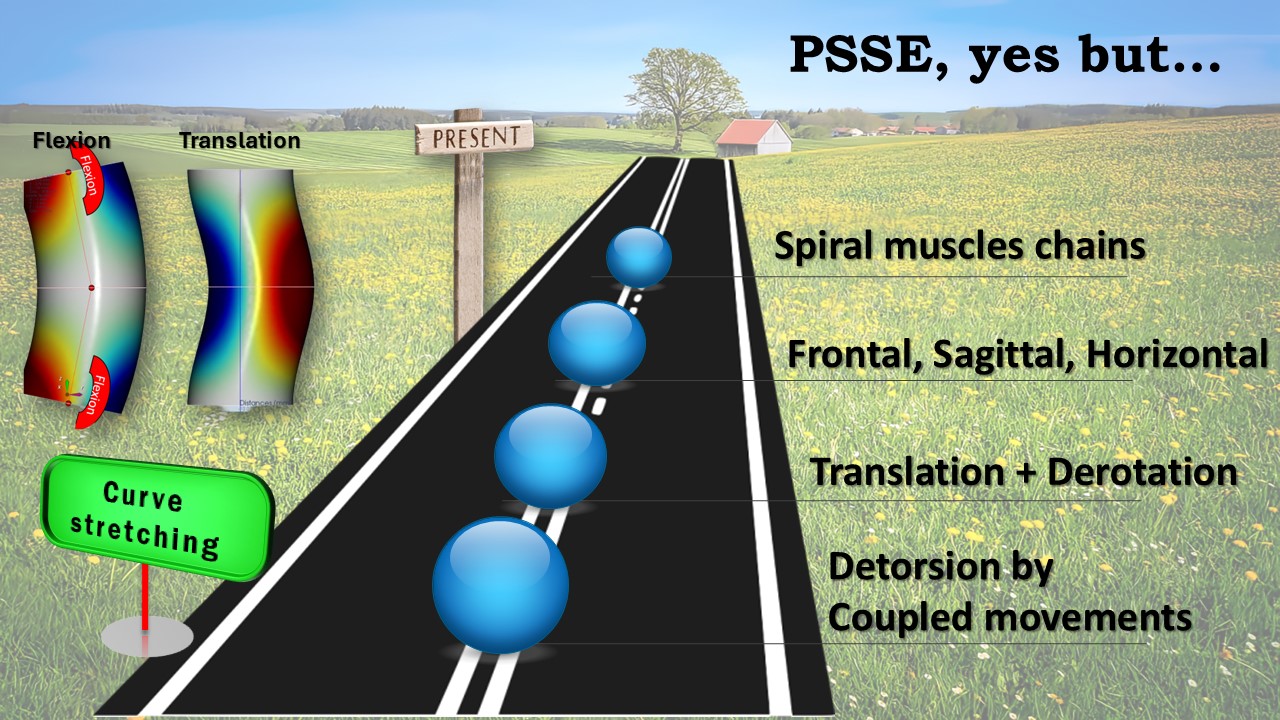 |
Beyond the realm of specific exercises, a significant consideration arises concerning the implementation of PSSE. One pertinent question is: how does one rectify the curve? Given that this is a three-dimensional deviation, countless possibilities exist. When looking at the frontal plane, the options boil down to flexion, which elongates the concavity, or translation, executed at a constant volume. The Lyon Method employs thoracic frontal flexion and lumbar translation in conjunction with sagittal normalization, facilitating mechanical detorsion at both thoracic and lumbar levels. On the other hand, the Schroth method integrates translation with derotation. Klapp adopts a methodical approach, gradually relaxing the body in all three planes, while FITS utilizes spiral muscle chains. Considering the unique nature of each scoliosis condition, it would be ideal to familiarize oneself with as many techniques as possible to select the most suitable one for the specific curve in question. |
 |
Acquiring proficiency in one or more techniques is crucial. Comparable to the comprehensive nature of a car, each method functions as an integrated system. The guidelines and indicators visible on the control panel for various methods may differ significantly. Furthermore, once the angulation rises above 20° during adolescence, it is common practice to pair physiotherapy with a brace. Many physiotherapy techniques have evolved to harmonize effectively with a particular type of brace. When the abgulation is below 20°, selecting a physiotherapy approach will be contingent upon the source of the condition, known as "idiopathic" scoliosis. |
 |
What leads to the development of idiopathic scoliosis? This perplexing question, often posed by concerned parents, is precisely what sparked the inception of the future. Although numerous studies have been conducted on this enigmatic condition, most explanations have remained incomplete and distinguishing between primary and secondary causes has proven elusive. The challenge of achieving a comprehensive synthesis is compounded by the fragmented perspectives offered by various medical specialties. |
 |
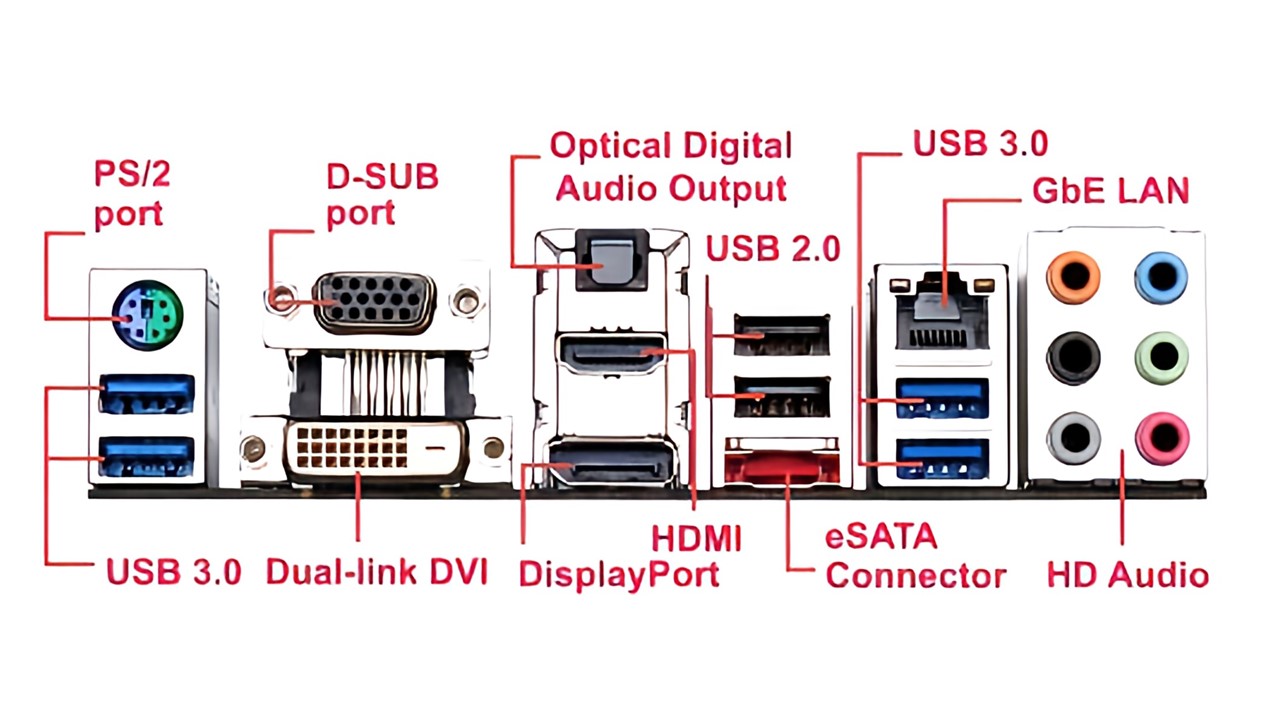
Scoliosis is a complex condition influenced by multiple factors, and to gain a clearer understanding of how these factors interact, it is helpful to liken them to a computer.
|
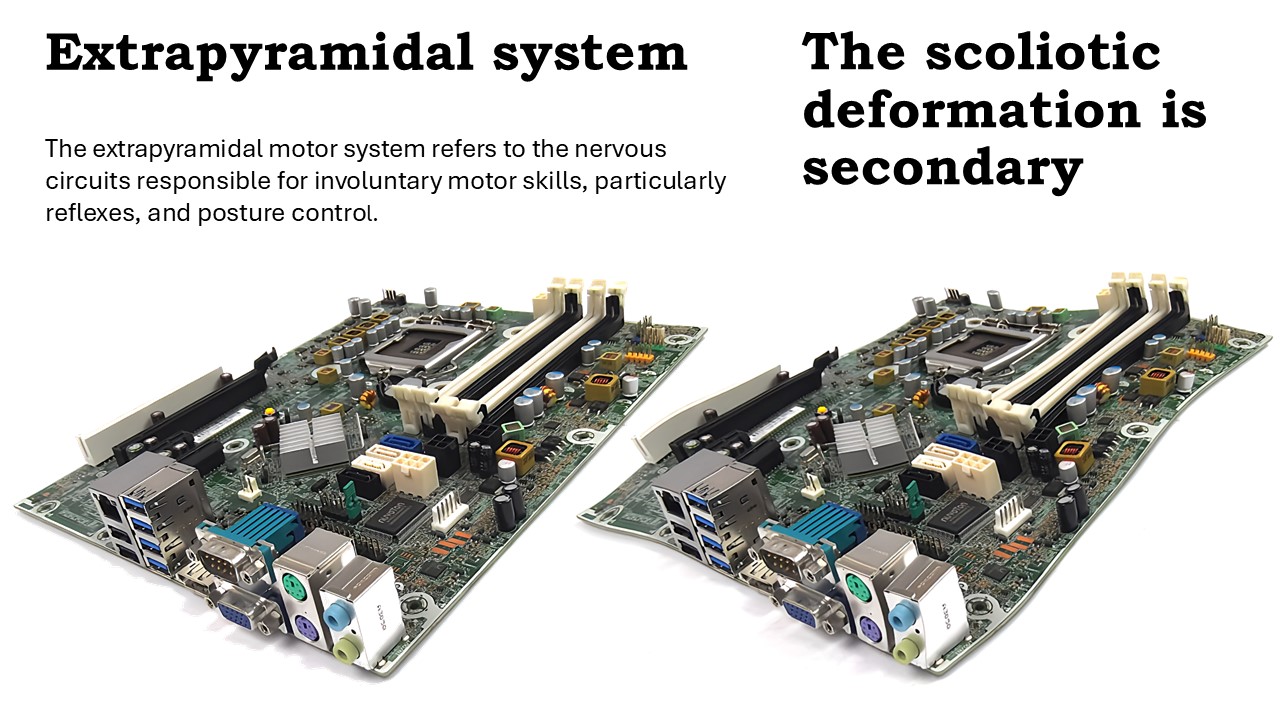 |
The extrapyramidal system is analogous to the motherboard of a computer. This system coordinates inputs and outputs, houses the internal clock, and enables the newborn to live and move. The voluntary pyramidal system is similar to the microprocessor. It controls the motherboard but does not eliminate its functions.
|
 |
In 2024, Grivas has come close to reaching a definitive conclusion. Through careful examination of school screenings, it has been hypothesized that alterations in vertebral growth associated with the onset of idiopathic scoliosis are not inherent but instead are secondary modifications. The root cause initiating the deformity does not reside within the vertebral bodies themselves. Rather, the distortions observed in these vertebrae are consequential results of uneven forces acting upon them. These forces arise from muscular pressure, growth dynamics, and the influence of gravity. |
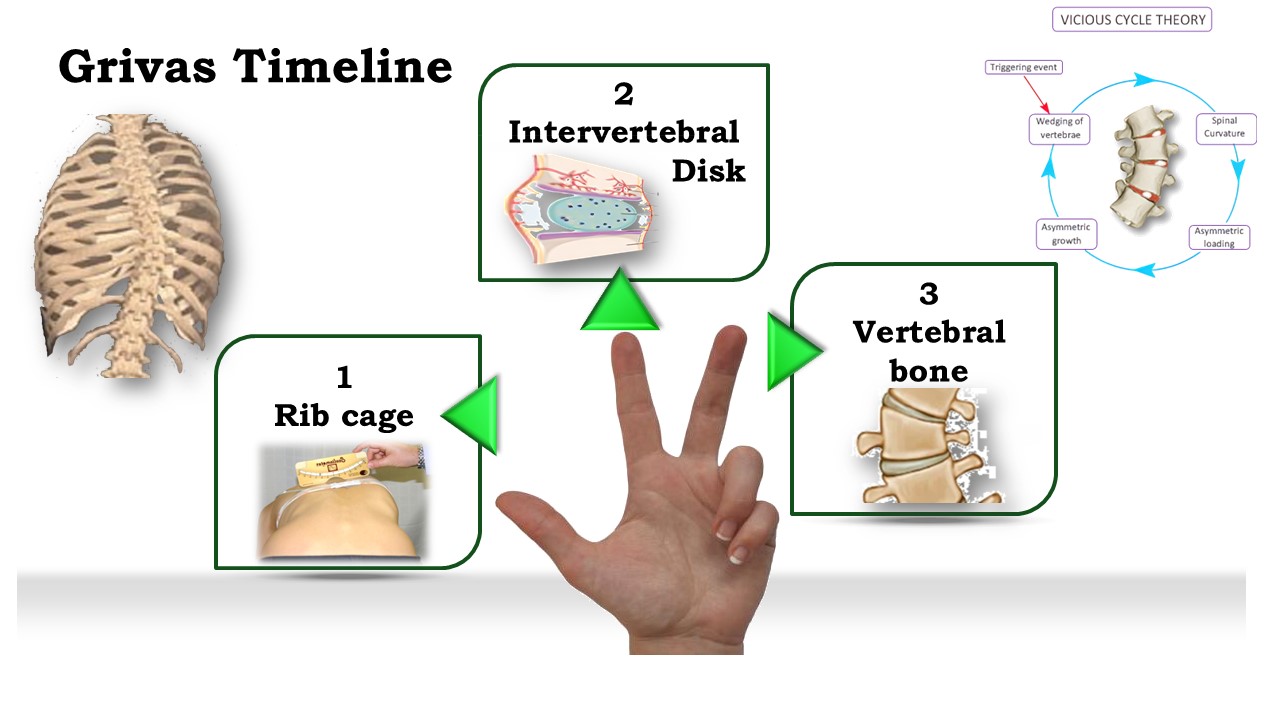 |
An in-depth examination of the school screening details the timeline of the deformations. In idiopathic scoliosis, the deformation first impacts the ribs, followed by the intervertebral disc, and ultimately the vertebral body. |
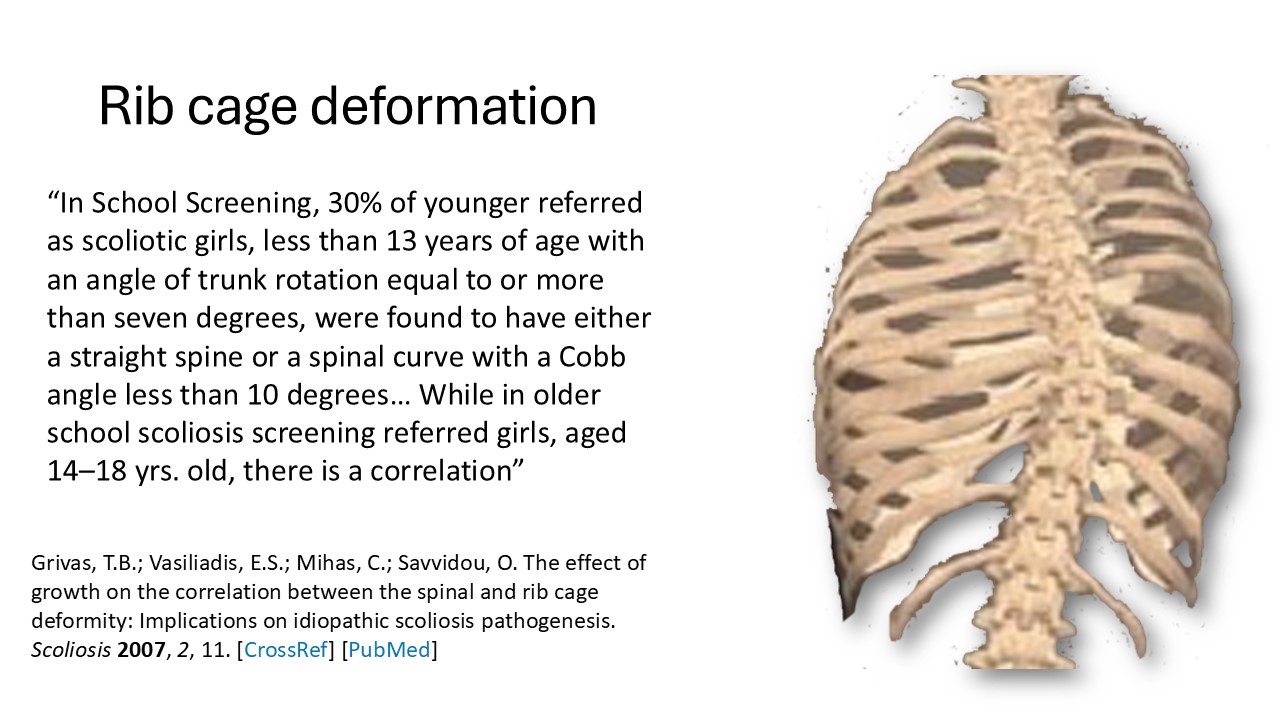 |
During a school screening process, it was observed that among younger girls referred for potential scoliosis—specifically those under the age of 13 exhibiting a trunk rotation angle of seven degrees or more—30% were actually found to either possess a straight spine or to have a spinal curvature with a Cobb angle measuring under 10 degrees. Conversely, in the case of older girls aged between 14 and 18 years who were referred through scoliosis screening, a discernible correlation was identified. |
 |
A tangible clinical application of this notion involves assessing the double costal contour index via profile radiography. When this index exceeds 1.5 at a minimal Cobb angle, it can serve as a predictor for future progression. |
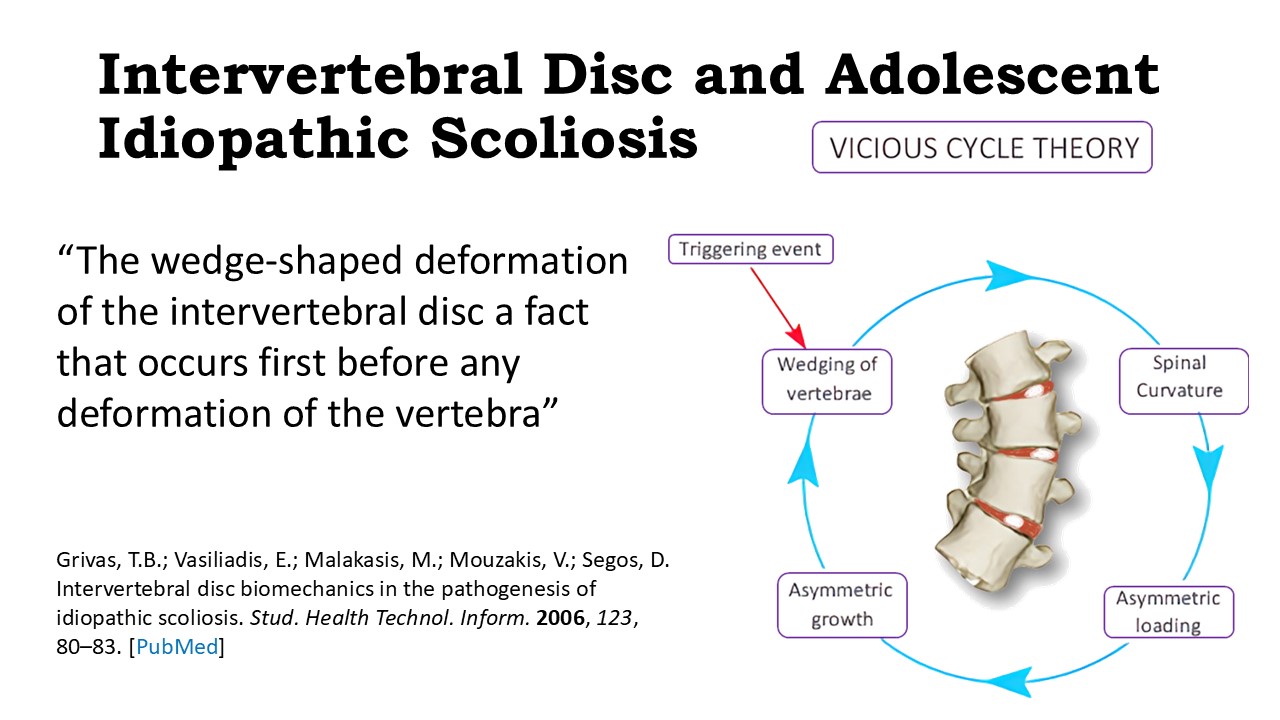 |
In a similar manner, the intervertebral disc undergoes deformation prior to any alteration in the structure of the vertebral body. Consequently, it can be concluded that bone deformation is not an initial occurrence. |
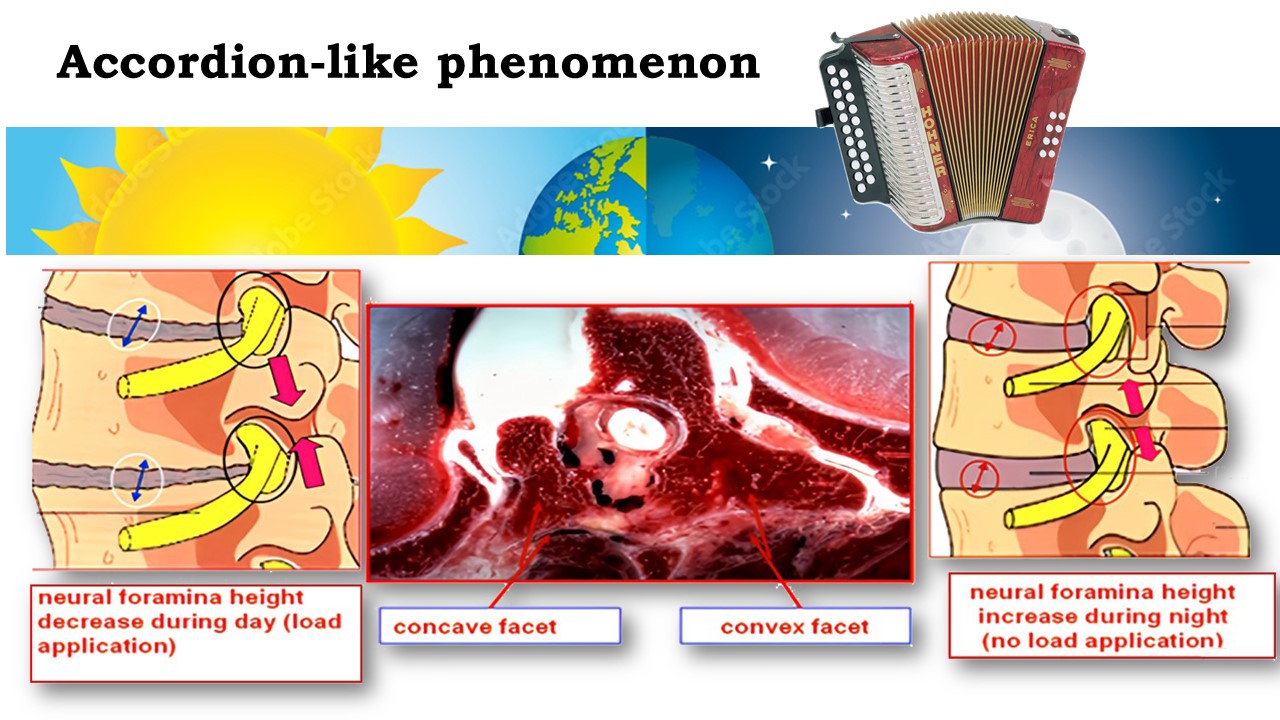 |
Throughout the day, the intervertebral disc undergoes compression, only to rehydrate during the nighttime hours. This movement, where the disc's nucleus shifts towards the area of convexity, serves as the fundamental principle behind the use of hypercorrective night braces for treatment. Nonetheless, these braces address merely one aspect of the broader consequences associated with scoliosis. |
 |
The reductionist method allows for a clear examination of the arguments supporting each factor as either primary or secondary. All factors, aside from the extrapyramidal system, are considered secondary. |
 |
The motherboard of a computer houses a crucial component known as the BIOS, which is an acronym for Basic Input/Output System. This BIOS is tasked with two primary roles. Firstly, it conducts an assessment to ensure that the motherboard components and connected peripherals, such as the keyboard and hard disk, are functioning correctly. Secondly, it is responsible for initiating the operating system. In a manner similar to the BIOS, the extrapyramidal system serves as an autonomous and involuntary network comprised of numerous afferents, autonomous processing centers, and four distinct tracts. These tracts are instrumental in managing functions such as muscle tone. At birth, the extrapyramidal system dominates motor control, yet over time, it is gradually overtaken by the voluntary pyramidal system. However, it continues to play a significant role at the trunk level, where it maintains its importance. |
 |
The motherboard's internal clock resembles that of humans, enabling adaptation to the day-night cycle.
|
 |
Melatonin exemplifies the most distinctive case. Its production peaks at night and during adolescence. Dubousset observed that lack of melatonin in chickens results in scoliosis. Similarly, Machida induced the same condition in rats. When the rats lose their front legs, they start walking on two legs, and scoliosis develops. However, if they continue to walk on four legs, scoliosis does not occur.
|
 |
A melatonin deficit at the cellular level causes a symptomatology very close to what is observed in scoliosis: Lack of postural control, vestibular and proprioceptive dysfunction, muscle tone anomalies, osteopenia, platelet anomalies with increase in calmodulin level. |
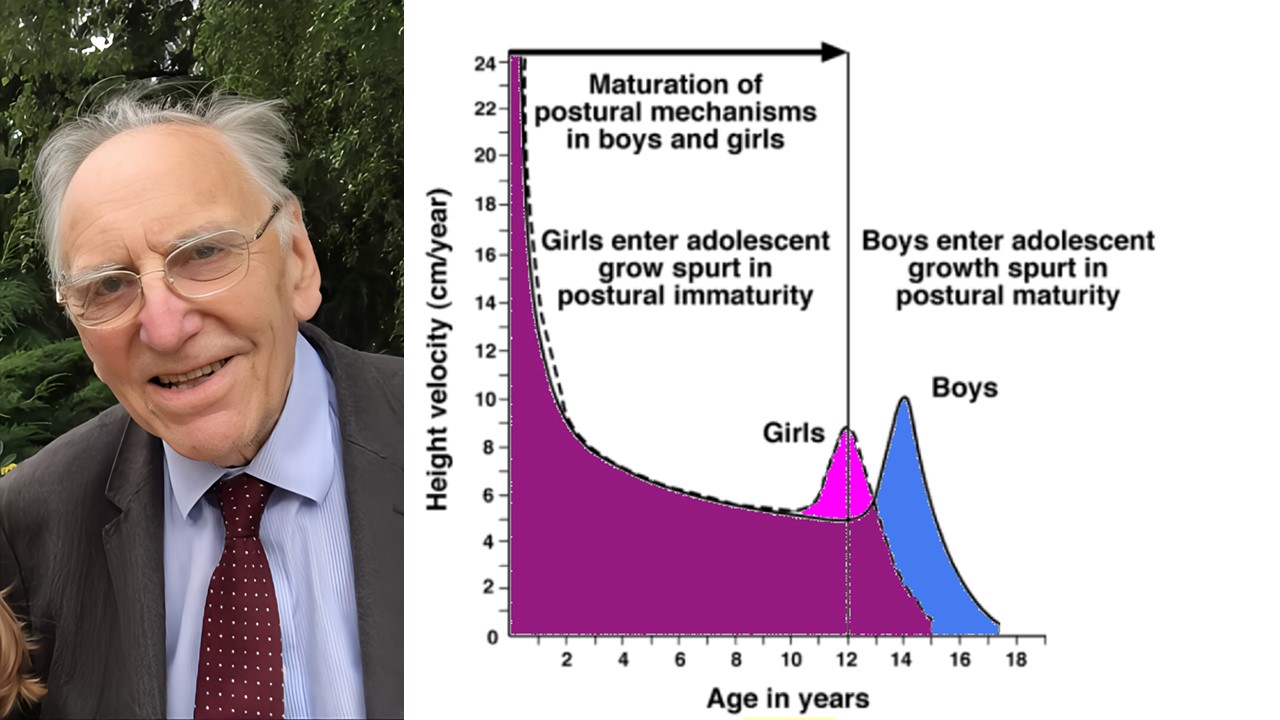 |
By the age of twelve, the proprioceptive receptors located within the vertebrae of humans have usually reached full maturity. Burwell suggests that scoliosis, particularly its higher prevalence among girls, can be attributed to a delayed maturation of the extrapyramidal system's afferent pathways. This difference of frequency may be linked to the earlier onset of pubertal growth in girls, which typically occurs two years before it does in boys. This phenomenon, known as Neuro-Osseous Timing of Maturation (NOTOM), offers a compelling explanation for the gender disparity observed in the development of scoliosis. |
 |
In 2023, Shen conducted a study examining three different groups of patients with scoliosis. The first group underwent a regimen that integrated both balance training and curve correction techniques. The second group received treatment focused solely on curve correction. Meanwhile, the third group did not participate in any form of physiotherapy. After a period of six weeks, the outcomes distinctly favored the first group, demonstrating significant improvements, as evidenced by a level 1 randomized controlled trial (RCT). |
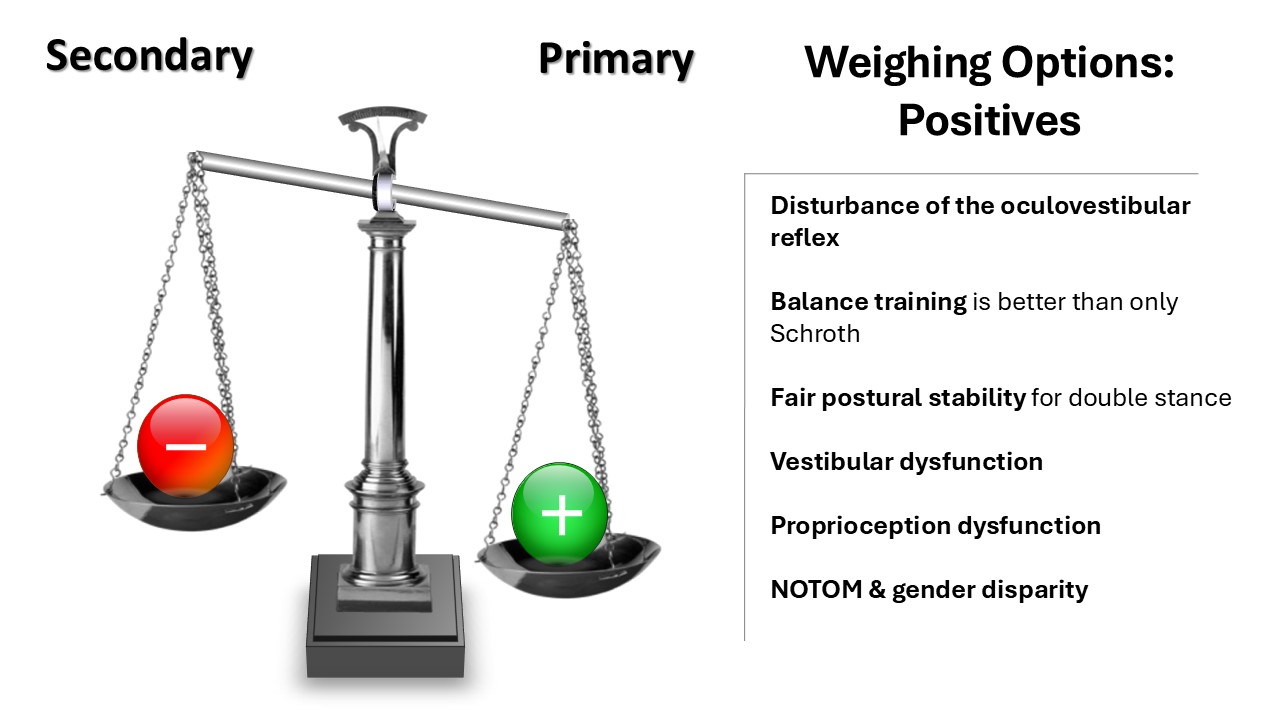 |
For many years, there have been significant and enduring arguments supporting the idea that the primary cause of scoliosis may be linked to the afferents of the extrapyramidal system. This theory is bolstered by observations such as disruptions in the oculo-vestibular reflex, the enhanced effectiveness of physiotherapy that includes balance training, and the noticeable impairments in postural stability, as well as vestibular and proprioceptive functions in individuals with scoliosis. Additionally, the delayed maturation of the postural system provides insight into why scoliosis is more prevalent in girls. |
 |
Systemic biology enables a deeper comprehension of how living systems interact with their surroundings. It is rooted in a mathematical framework that combines biological data and facilitates the definition of biological models. |
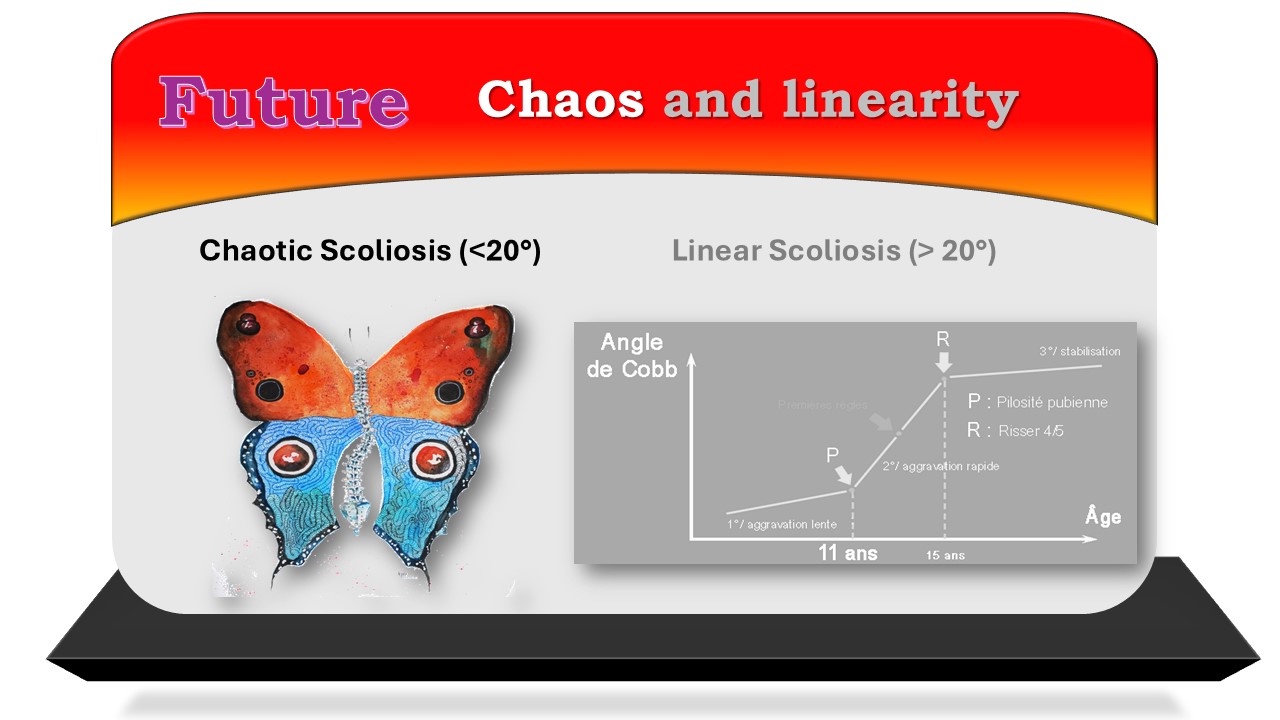 |
The Lyon Method describes two biological models in the development of scoliosis. For scoliosis under 20°, the chaotic model applies, while the linear model is used for scoliosis over 20°. The chaotic model is linked to the extrapyramidal origin of scoliosis. |
 |
Scoliosis exemplifies the chaos theory as it relates to the spinal column. The system is: open (maintaining an upright posture and interacting with the external environment), non-predictive (akin to the butterfly effect), complex (involving multiple factors), discontinuous (occurring in stages), deterministic (not random), moldable (involving a fourth fractal dimension), with a strange attractor, and undergoes changes in physiological behavior during puberty. |
 |
The foundation of chaos theory in mathematics is the fractal dimension present in humans. Leonardo da Vinci's anatomical sketches of the spine enable us to discover the golden ratio by calculating the division of lordosis with kyphosis. When 63 is divided by 39, the result is 1.618. This ratio is similarly found in the proportions of the vertebral body and the configuration of the intervertebral disc. |
 |
The initial paradigm shift involves physiotherapy for treating scoliosis with a curvature of less than 25°. When the spinal deviation results from a defect in the extrapyramidal system, physiotherapy should focus on stimulating the afferents and efferents of this system. Corrective exercises for the deviation are considered secondary. |
 |
The resilience of the basal ganglia is noteworthy, and there are many ways they compensate; thus, physiotherapy targets the afferents and efferents of the extrapyramidal system. |
 |
The extrapyramidal system is essential for maintaining various body postures and enabling transitions between them. Posture regulation is mainly controlled by three vital systems: ocular, vestibular, and proprioceptive muscle and joint systems. In the case of scoliosis, special attention is given to spinal proprioception. |
 |
In the skin along the midline of the spinous process, there are numerous proprioceptive receptors. Ruffini corpuscles are responsive to pressure and skin stretching. Pacini corpuscles, which are fast-adapting mechanoreceptors, detect strong and sustained pressure. Meissner corpuscles sense vibrations or movements. |
 |
Exercise 2 of the Lyon Method stimulates Ruffini corpuscles by stretching during kyphosis, which is particularly suitable for a flat back. |
 |
The third exercise of the Lyon Method activates Pacini corpuscles by performing gradual, deep stretches beginning at the midline and extending the abdomen toward the ribs. |
 |
The mobilization process occurs at the convex region, which serves as a stable anchor, and at the concave area, through lifting and rotating actions. |
 |
If the angulation is greater than 20°, axial stretching can be combined with opening of the thoracic concavity. |
 |
The efferent pathways of the extrapyramidal system comprise four distinct tracts. While these are present at birth, they mature at different stages, and physiotherapy should align with this developmental process. The reticulospinal tract is engaged from birth until five years, the vestibulospinal tract develops between five and seven years, the tectospinal tract from seven to nine years, and lastly, the rubrospinal tract matures. |
 |
You don't have to be a specialist in psychomotor therapy; the exercises are quite straightforward. For newborns with scoliosis, prior to them learning to walk, perform flexion-extension exercises while keeping the alignment from the C7 to S2 straight, followed by lateral tilting exercises towards the inward curve. While the child is on their stomach, extend the arm on the concave side using a toy. |
 |
Once a child begins to walk, a beam with minor obstacles placed on the ground is introduced. Additionally, a path featuring footprints and handprints can be utilized.
|
 |
Starting at age seven, children can mimic the movements of their arms and legs, initially in the same direction and later in opposing directions. This aligns with the right side of each participant when they face one another.
|
 |
The stimulation of the rubrospinal tract begins at age ten through activities focusing on fine motor skills, as well as improving speed and coordination across all four limbs. |
 |
No matter what the scoliosis angle is, the final four exercises in the Lyon Method are designed to specifically focus on the four pathways of the extrapyramidal system. |
 |
The evaluation of physiotherapy for the extrapyramidal system can be objectively assessed. For instance, using the Huber device allows monitoring physiotherapy progress through seven different tests. |
 |
The next paradigm shift relates to the source of spinal deformation occurring at the intervertebral disc level. For scoliosis measuring 20 to 30°, exercises performed while lying down or on all fours (Klapp method) will help maintain the intervertebral disc. |
 |
For angulations under 40°, the main drawback of surgery is that it obstructs the intervertebral discs, while non-surgical treatments target the disc directly through the ribs. |
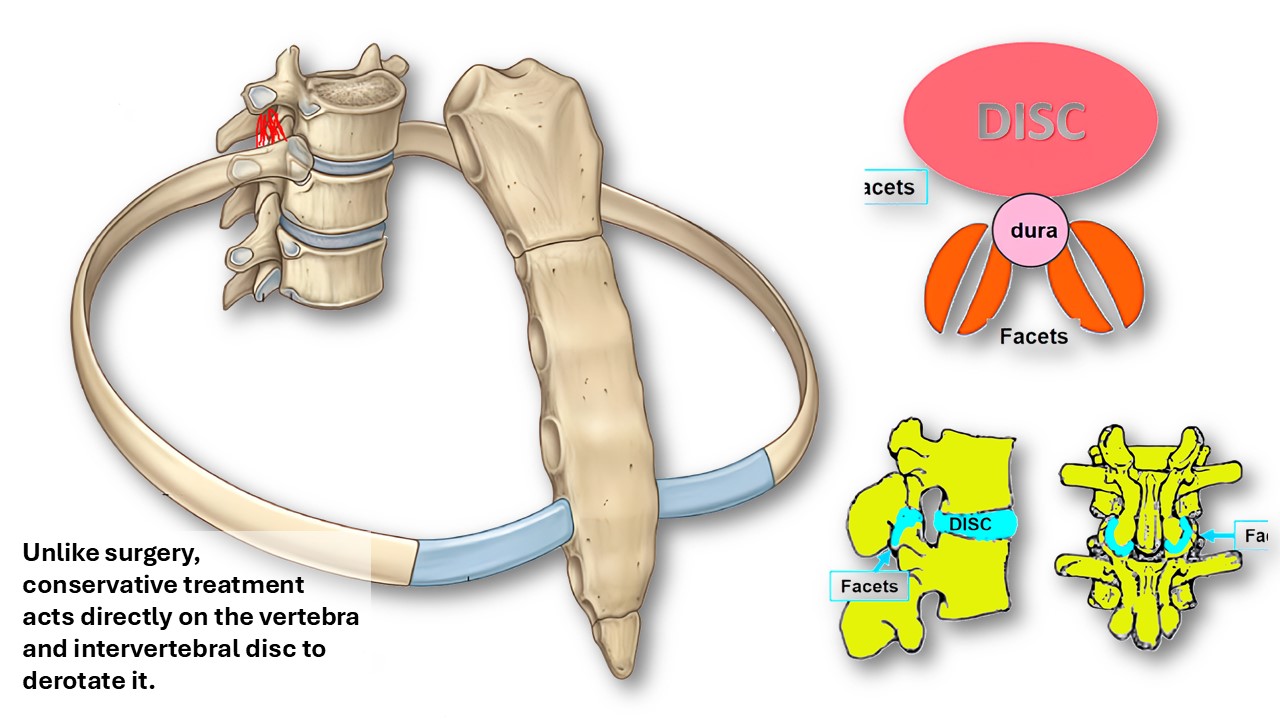 |
The rib's neck is positioned at the level of the intervertebral disc and transverse process in an anatomical context. This positioning is the reason for the Lyon Method's focus on sagittal isostatic balance, aiming to distribute pressure evenly between the intervertebral disc in the front and the posterior facets. |
 |
Exercise No. 4 of the Lyon Method is carried out in a supine position and primarily targets the costovertebral junction. Segmental mobilization is executed at two distinct levels, on both the outward and inward curvatures, to facilitate vertebral mobilization. The thumb is positioned directly on the convex side of the transverse process and the middle finger on the concave side. The skin planes are extended between the convex and concave areas. |
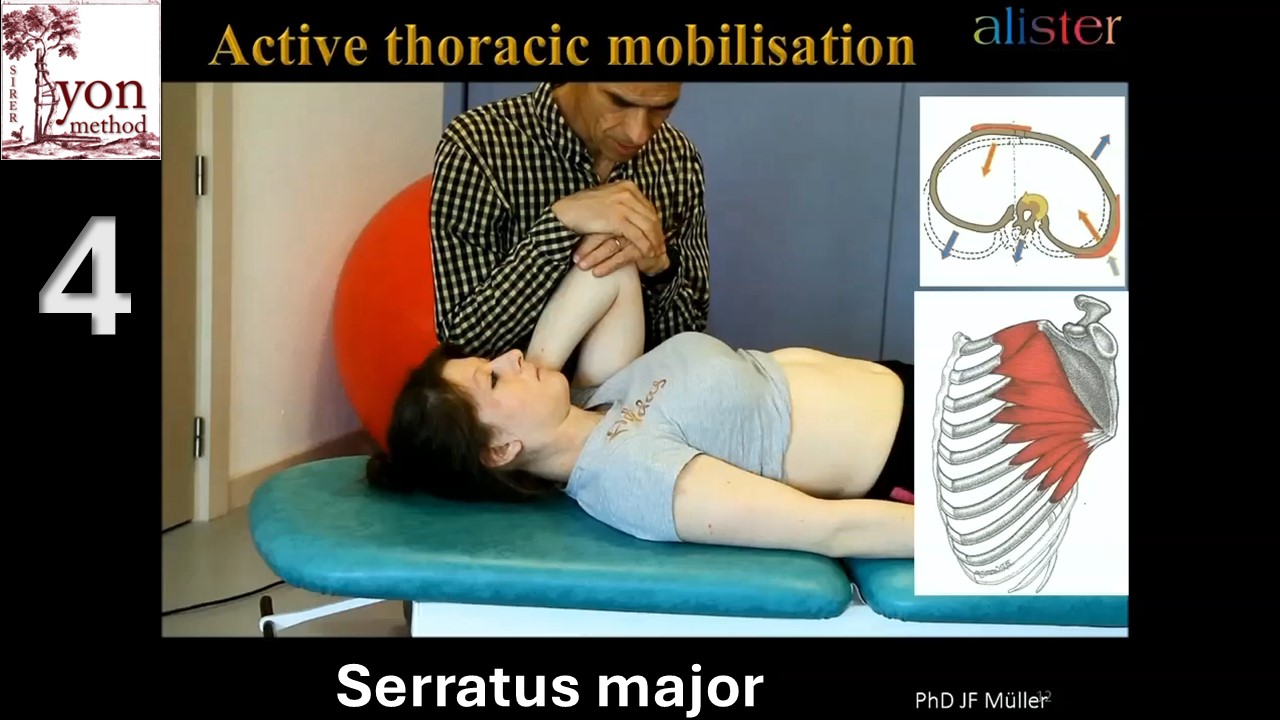 |
An adaptation of activity number 4 effectively demonstrates derotation via concavity. This is achieved passively by the shoulder blade and actively by contracting the serratus anterior. |
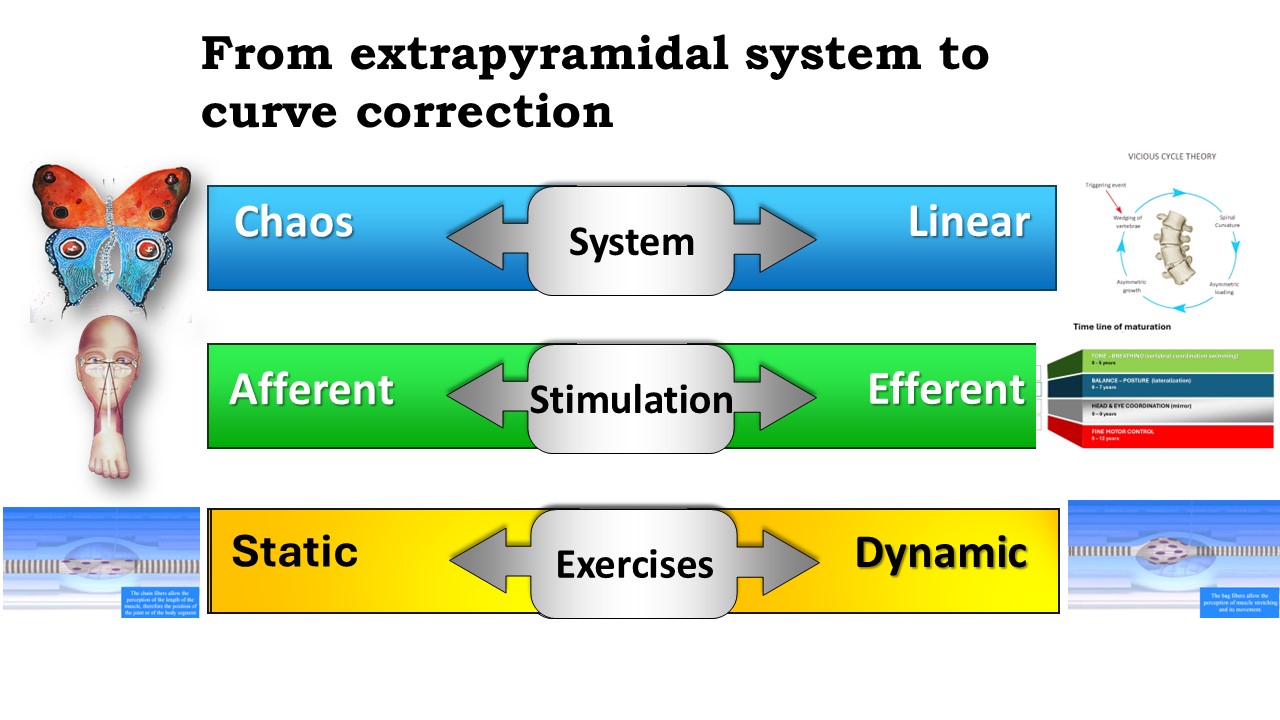 |
The physiotherapy approach to scoliosis varies with the degree of the condition's curvature, focusing on assessing the stimulation of the extrapyramidal system alongside efforts to rectify the curve. These exercises target both afferent and efferent pathways, tailored to their level of development through static and dynamic movements.
|
